

The impact of simultaneous liver resection for occult liver metastases of pancreatic adenocarcinoma
- PMID: 23258977
- PMCID: PMC3508736
- DOI: 10.1155/2012/939350
The impact of simultaneous liver resection for occult liver metastases of pancreatic adenocarcinoma
Abstract
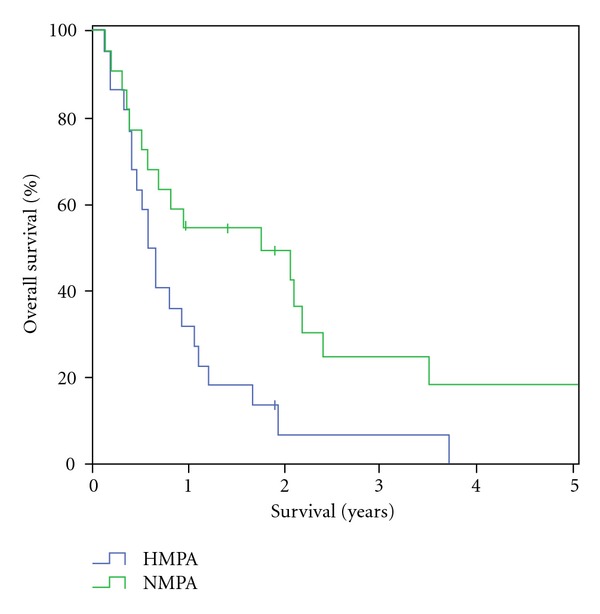
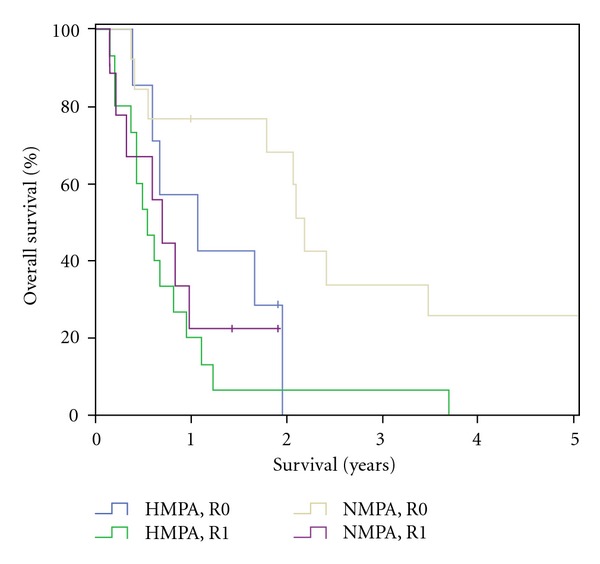
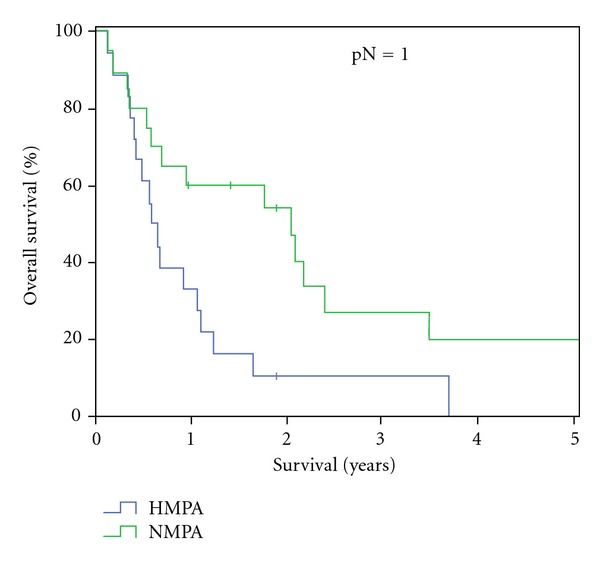
Backround. Pancreas resection is the only curative treatment for pancreatic adenocarcinoma. In the event of unexpected incidental liver metastases during operative exploration patients were traditionally referred to palliative treatment arms. With continuous progress in the surgical expertise simultaneous pancreas and liver resections seem technically feasible nowadays. The aim of this study therefore was to analyze the impact of synchronous liver-directed therapy on operative outcome and overall survival in patients with hepatic metastasized pancreatic adenocarcinoma (HMPA). Methods. 22 patients who underwent simultaneous pancreas resection and liver-directed therapy for HMPA between January 1, 2004 and January 1, 2009 were compared to 22 patients who underwent classic pancreas resection for nonmetastasized pancreatic adenocarcinoma (NMPA) in a matched pair study design. Postoperative morbidity, preoperative, and operative data and overall survival were analyzed. Results. Overall survival was significantly decreased in the HMPA group. Postoperative morbidity and mortality and median operation time did not significantly differ between the groups. Conclusion. The results of our study showed that simultaneous pancreas resection and liver-directed therapy may safely be performed and may therefore be applied in individual patients with HMPA. However, a potential benefit of this radical surgical approach with regard to overall survival and/or quality of life remains to be proven.
Figures
References
-
- Bradley EL. Long-term survival after pancreatoduodenectomy for ductal adenocarcinoma the emperor has no clothes? Pancreas. 2008;37(4):349–351. - PubMed
-
- Dimagno EP, Reber HA, Tempero MA. AGA technical review on the epidemiology, diagnosis, and treatment of pancreatic ductal adenocarcinoma. Gastroenterology. 1999;117(6):1464–1484. - PubMed
-
- Neoptolemos JP, Dunn JA, Stocken DD, et al. Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer: a randomised controlled trial. The Lancet. 2001;358(9293):1576–1585. - PubMed
-
- Kim RD, Kundhal PS, McGilvray ID, et al. Predictors of failure after pancreaticoduodenectomy for ampullary carcinoma. Journal of the American College of Surgeons. 2006;202(1):112–119. - PubMed
LinkOut - more resources
Full Text Sources
