

Combination of infliximab and high-dose intravenous immunoglobulin for toxic epidermal necrolysis: successful treatment of an elderly patient
- PMID: 23259092
- PMCID: PMC3505931
- DOI: 10.1155/2012/915314
Combination of infliximab and high-dose intravenous immunoglobulin for toxic epidermal necrolysis: successful treatment of an elderly patient
Abstract
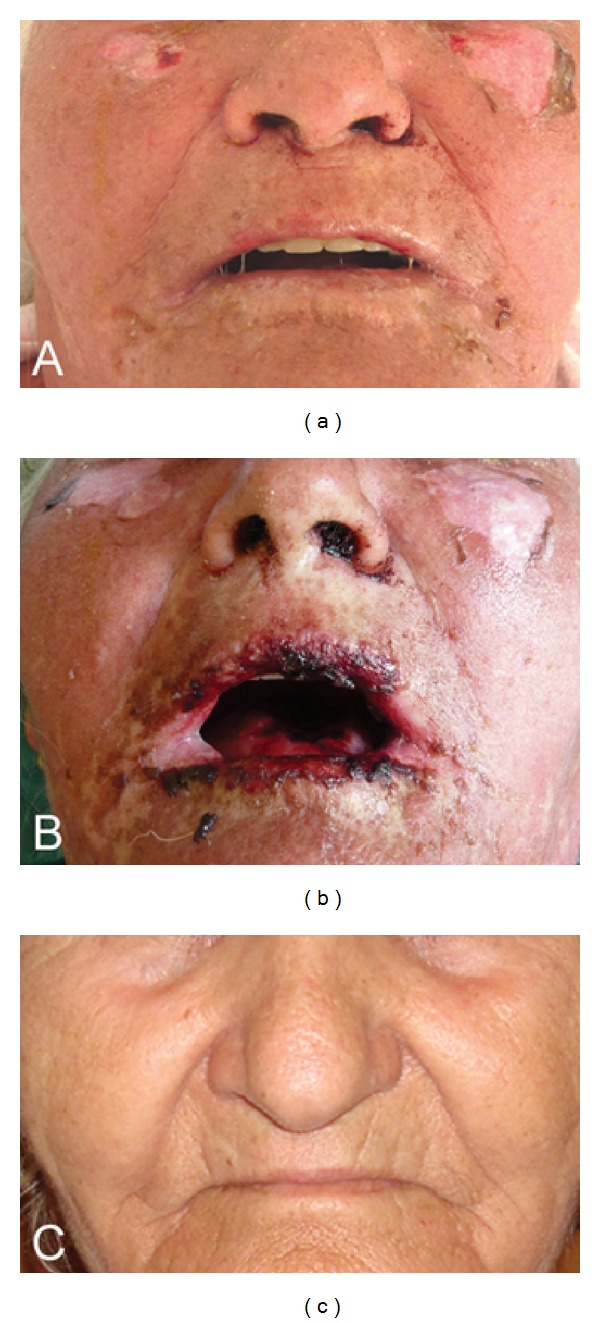
Toxic epidermal necrolysis (TEN) is a rare, severe cutaneous adverse drug reaction with average mortality 25-35%, especially among elderly multimorbid patients. Established therapeutic guidelines do not exist and controversies underlie many of the presently suggested treatment regimens. Herein we present the use of the recently described combination scheme of methylprednisolone (500 mg methylprednisolone bolus i.v.) followed by infliximab (5 mg/kg i.v.) and high-dose intravenous immunoglobulin (2 g/kg over 5 days) to treat an elderly, 74-year-old female patient with TEN (SCORTEN 3) within the premises of a district hospital. Already from the second day of hospitalization the skin condition markedly stabilized and the patient's status improved rapidly thereafter. She was discharged after 19 days in stationary care in excellent general condition and remained without any sequels 9 months afterwards. The present paper further supports the feasibility, efficacy, and safety of the proposed combination modality for the treatment of elderly patients with TEN, a population susceptible to more severe TEN.
Figures
References
-
- Downey A, Jackson C, Harun N, Cooper A. Toxic epidermal necrolysis: review of pathogenesis and management. Journal of the American Academy of Dermatology. 2012;66(6):995–1003. - PubMed
-
- Lissia M, Mulas P, Bulla A, Rubino C. Toxic epidermal necrolysis (Lyell’s disease) Burns. 2010;36(2):152–163. - PubMed
-
- Prins C, Kerdel FA, Padilla RS, et al. Treatment of toxic epidermal necrolysis with high-dose intravenous immunoglobulins: multicenter retrospective analysis of 48 consecutive cases. Archives of Dermatology. 2003;139(1):26–32. - PubMed
-
- Gaitanis G, Spyridonos P, Patmanidis K, et al. Treatment of toxic epidermal necrolysis with the combination of infliximab and high-dose intravenous immunoglobulin. Dermatology. 2012;224:134–139. - PubMed
-
- Wolkenstein P, Latarjet J, Roujeau JC, et al. Randomised comparison of thalidomide versus placebo in toxic epidermal necrolysis. The Lancet. 1998;352(9140):1586–1589. - PubMed
LinkOut - more resources
Full Text Sources
