

Staphylococcal infections in children, California, USA, 1985-2009
- PMID: 23260060
- PMCID: PMC3557972
- DOI: 10.3201/eid1901.111740
Staphylococcal infections in children, California, USA, 1985-2009
Abstract
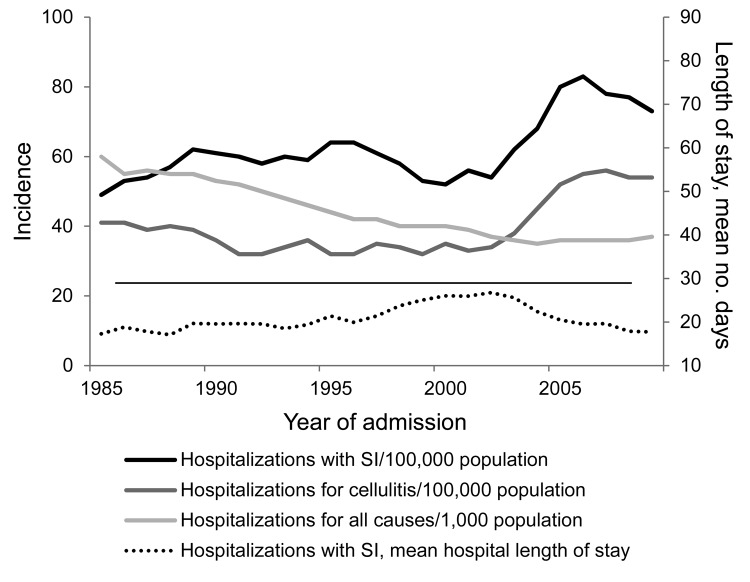
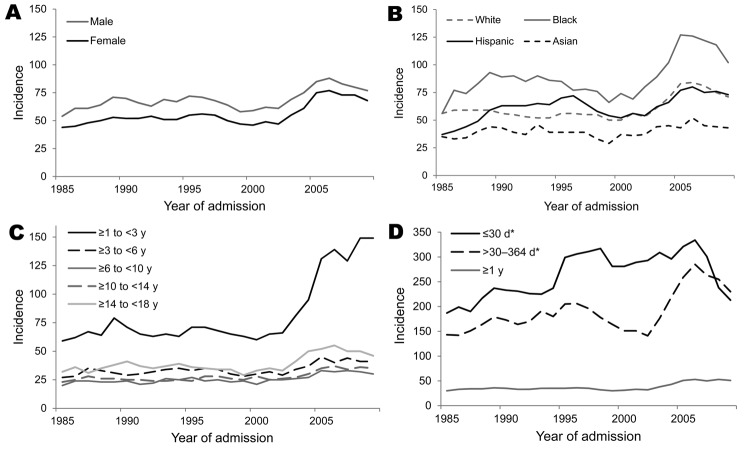
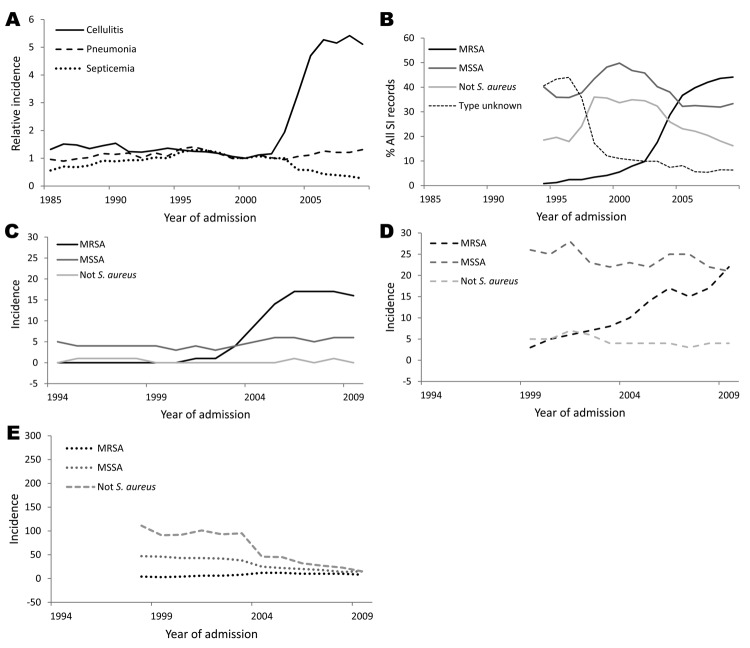
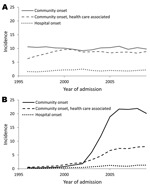
We conducted a retrospective, observational, population-based study to investigate the effect of staphylococcal infections on the hospitalization of children in California during 1985-2009. Hospitalized children with staphylococcal infections were identified through the California Office of Statewide Health Planning and Development discharge database. Infections were categorized as community onset, community onset health care-associated, or hospital onset. Infection incidence was calculated relative to all children and to those hospitalized in acute-care facilities. A total of 140,265 records were analyzed. Overall incidence increased from 49/100,000 population in 1985 to a peak of 83/100,000 in 2006 and dropped to 73/100,000 in 2009. Staphylococcal infections were associated with longer hospital stays and higher risk for death relative to all-cause hospitalizations of children. The number of methicillin-resistant Staphylococcus aureus infections increased, and the number of methicillin-susceptible S. aureus infections remained unchanged. Children <3 years of age, Blacks, and those without private insurance were at higher risk for hospitalization.
Figures
Similar articles
-
Children with atopic dermatitis appear less likely to be infected with community acquired methicillin-resistant Staphylococcus aureus: the San Diego experience.Pediatr Dermatol. 2011 Jan-Feb;28(1):6-11. doi: 10.1111/j.1525-1470.2010.01293.x. Epub 2010 Nov 11. Pediatr Dermatol. 2011. PMID: 21070347
-
Staphylococcus aureus bloodstream infections: risk factors, outcomes, and the influence of methicillin resistance in Calgary, Canada, 2000-2006.J Infect Dis. 2008 Aug 1;198(3):336-43. doi: 10.1086/589717. J Infect Dis. 2008. PMID: 18522502
-
Increasing role of Staphylococcus aureus and community-acquired methicillin-resistant Staphylococcus aureus infections in the United States: a 10-year trend of replacement and expansion.Microb Drug Resist. 2011 Jun;17(2):321-8. doi: 10.1089/mdr.2010.0193. Epub 2011 Mar 19. Microb Drug Resist. 2011. PMID: 21417776
-
Epidemiology of methicillin-resistant Staphylococcus aureus.Clin Infect Dis. 2008 Jun 1;46 Suppl 5:S344-9. doi: 10.1086/533590. Clin Infect Dis. 2008. PMID: 18462089 Review.
-
Current challenges in treating MRSA: what are the options?Expert Rev Anti Infect Ther. 2008 Oct;6(5):601-18. doi: 10.1586/14787210.6.5.601. Expert Rev Anti Infect Ther. 2008. PMID: 18847401 Review.
Cited by
-
Decreasing Incidence of Skin and Soft Tissue Infections With a Seasonal Pattern at an Academic Medical Center, 2006-2014.Open Forum Infect Dis. 2016 Aug 30;3(4):ofw179. doi: 10.1093/ofid/ofw179. eCollection 2016 Oct. Open Forum Infect Dis. 2016. PMID: 28852669 Free PMC article.
-
Update on Epidemiology and Treatment of MRSA Infections in Children.Curr Pediatr Rep. 2013 Sep 1;1(3):170-181. doi: 10.1007/s40124-013-0023-7. Curr Pediatr Rep. 2013. PMID: 24040579 Free PMC article.
-
Novel Inhibitor Discovery of Staphylococcus aureus Sortase B and the Mechanism Confirmation via Molecular Modeling.Molecules. 2018 Apr 23;23(4):977. doi: 10.3390/molecules23040977. Molecules. 2018. PMID: 29690584 Free PMC article.
-
Incidence of methicillin-resistant Staphylococcus aureus infection in a children's hospital in the Washington metropolitan area of the United States, 2003 - 2010.Emerg Microbes Infect. 2013 Oct;2(10):e69. doi: 10.1038/emi.2013.69. Epub 2013 Oct 9. Emerg Microbes Infect. 2013. PMID: 26038439 Free PMC article.
-
Characteristics and risk factors of hospital acquired - Methicillin-resistant Staphylococcus aureus (HA-MRSA) infection of pediatric patients in a tertiary care hospital in Riyadh, Saudi Arabia.Int J Pediatr Adolesc Med. 2016 Jun;3(2):71-77. doi: 10.1016/j.ijpam.2016.03.006. Epub 2016 Jun 8. Int J Pediatr Adolesc Med. 2016. PMID: 30805471 Free PMC article.
References
-
- King MD, Humphrey BJ, Wang YF, Kourbatova EV, Ray SM, Blumberg HM. Emergence of community-acquired methicillin-resistant Staphylococcus aureus USA 300 clone as the predominant cause of skin and soft-tissue infections. Ann Intern Med. 2006;144:309–17 . - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical