

Evaluation of the liver injury unit scoring system to predict survival in a multinational study of pediatric acute liver failure
- PMID: 23260095
- PMCID: PMC3786160
- DOI: 10.1016/j.jpeds.2012.11.021
Evaluation of the liver injury unit scoring system to predict survival in a multinational study of pediatric acute liver failure
Abstract
Objective: To examine the predictive value of the Liver Injury Units (LIU) and admission values (aLIU) of bilirubin and prothrombin time and international normalized ratio scores in a large cohort from the Pediatric Acute Liver Failure (PALF) Study Group, a multinational prospective study.
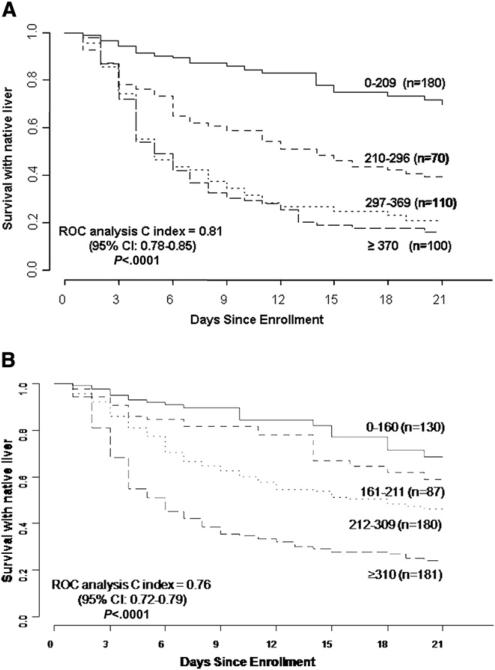
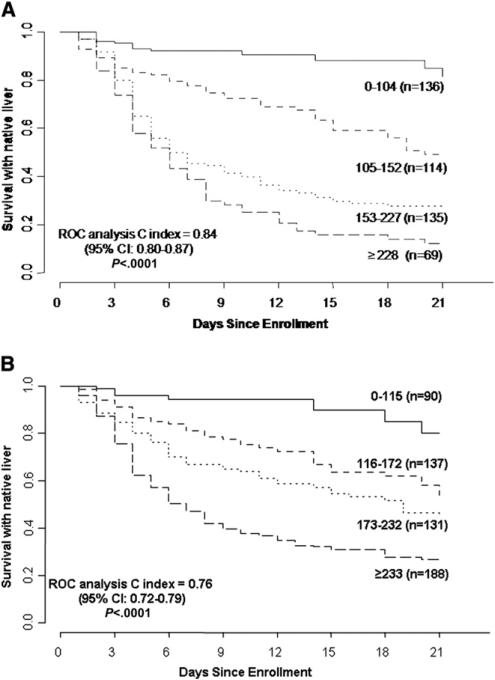
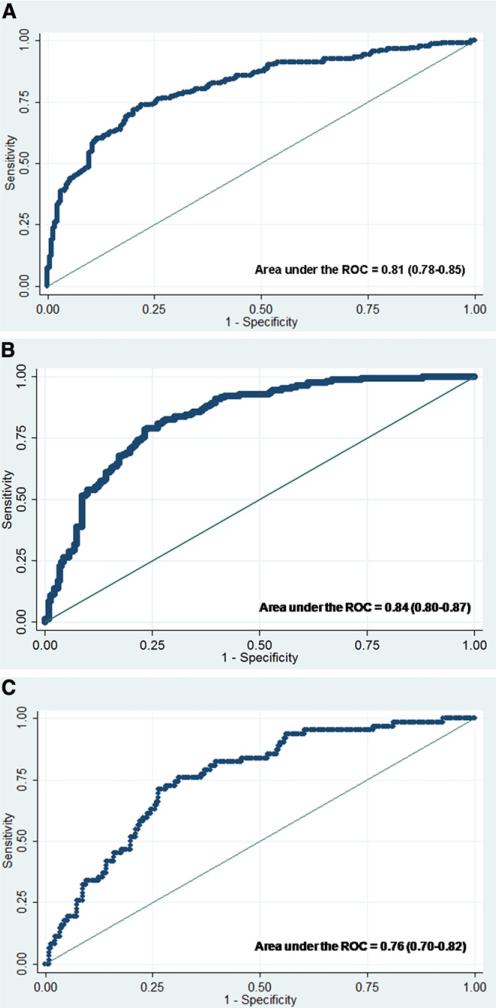
Study design: LIU and aLIU scores were calculated for 461 and 579 individuals, respectively, enrolled in the PALF study from 1999 to 2008. Receiver operator characteristic curves were used to evaluate the scores with respect to survival without liver transplantation (LT), death, or LT by 21 days after enrollment.
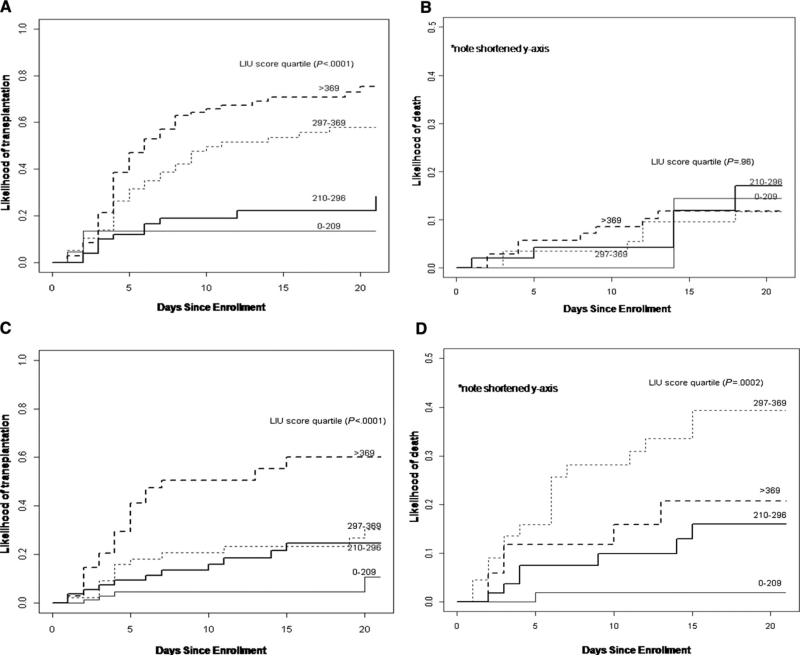
Results: At 21 days, 50.3% of participants were alive without LT, 36.2% underwent LT, and 13.4% died. The c-indices for transplant-free survival were 0.81 based on the LIU score with the international normalized ratio (95% CI, 0.78-0.85) and 0.76 based on the aLIU score (95% CI, 0.72-0.79). The LIU score predicted LT better than it predicted death (c-index for LT 0.84, c-index for death 0.76).
Conclusion: Based on data from a large, multicenter cohort of patients with PALF, the LIU score was a better predictor of transplant-free survival than was the aLIU score. The LIU score might be a helpful, dynamic tool to predict clinical outcomes in patients with PALF.
Copyright © 2013 Mosby, Inc. All rights reserved.
Figures
References
-
- Squires RH. Acute liver failure in children. Semin Liver Dis. 2008;28:153–66. - PubMed
-
- Liu E, MacKenzie T, Dobyns EL, Parikh CR, Karrer FM, Narkewicz MR, et al. Characterization of acute liver failure and development of a continuous risk of death staging system in children. J Hepatol. 2006;44:134–41. - PubMed
-
- Lee WS, McKiernan P, Kelly DA. Etiology, outcome and prognostic indicators of childhood fulminant hepatic failure in the United Kingdom. J Pediatr Gastroenterol Nutr. 2005;40:575–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
