

Is passive diagnosis enough? The impact of subclinical disease on diagnostic strategies for tuberculosis
- PMID: 23262515
- PMCID: PMC3733406
- DOI: 10.1164/rccm.201207-1217OC
Is passive diagnosis enough? The impact of subclinical disease on diagnostic strategies for tuberculosis
Abstract
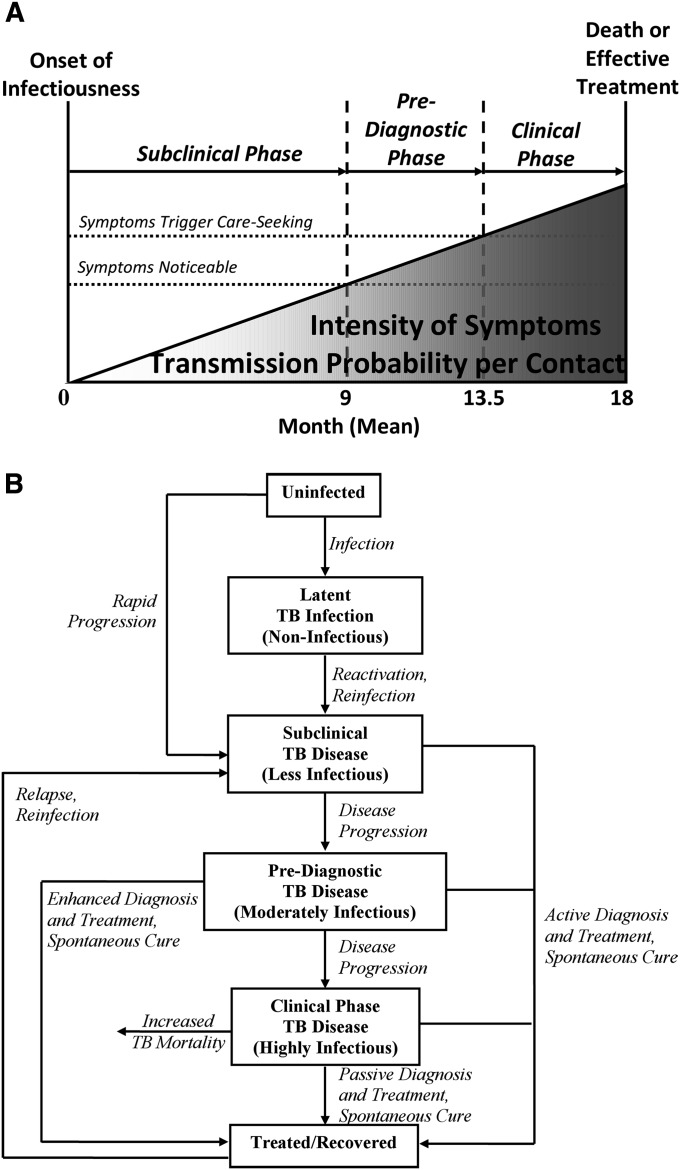
Rationale: Tuberculosis (TB) is characterized by a subclinical phase (symptoms absent or not considered abnormal); prediagnostic phase (symptoms noticed but diagnosis not pursued); and clinical phase (care actively sought). Diagnostic capacity during these phases is limited.
Objectives: To estimate the population-level impact of TB case-finding strategies in the presence of subclinical and prediagnostic disease.
Methods: We created a mathematical epidemic model of TB, calibrated to global incidence. We then introduced three prototypical diagnostic interventions: increased sensitivity of diagnosis in the clinical phase by 20% ("passive"); early diagnosis during the prediagnostic phase at a rate of 10% per year ("enhanced"); and population-based diagnosis of 5% of undiagnosed prevalent cases per year ("active").
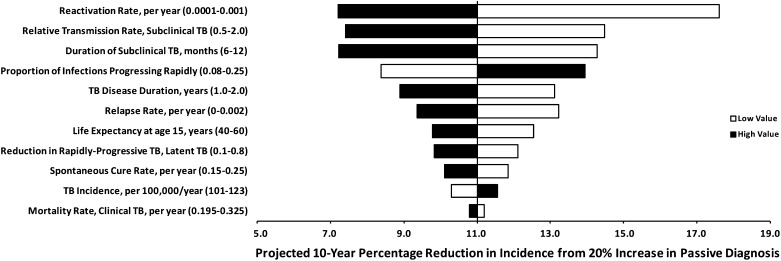
Measurements and main results: If the subclinical phase was ignored, as in most models, the passive strategy was projected to reduce TB incidence by 18% (90% uncertainty range [UR], 11-32%) by year 10, compared with 23% (90% UR, 14-35%) for the enhanced strategy and 18% (90% UR, 11-28%) for the active strategy. After incorporating a subclinical phase into the model, consistent with population-based prevalence surveys, the active strategy still reduced 10-year TB incidence by 16% (90% UR, 11-28%), but the passive and enhanced strategies' impact was attenuated to 11% (90% UR, 8-25%) and 6% (90% UR, 4-13%), respectively. The degree of attenuation depended strongly on the transmission rate during the subclinical phase.
Conclusions: Subclinical disease may limit the impact of current diagnostic strategies for TB. Active detection of undiagnosed prevalent cases may achieve greater population-level TB control than increasing passive case detection.
Figures
References
-
- Stop TB. Partnership. The global plan to stop TB, 2011–2015. Transforming the fight: towards elimination of tuberculosis. Geneva: World Health Organization; 2011.
-
- Dye C, Garnett GP, Sleeman K, Williams BG. Prospects for worldwide tuberculosis control under the WHO DOTS strategy. Lancet 1998;352:1886–1891 - PubMed
-
- Komatsu R, Korenromp EL, Low-Beer D, Watt C, Dye C, Steketee RW, Nahlen BL, Lyerla R, Garcia-Calleja JM, Cutler J, et al. Lives saved by Global Fund-supported HIV/AIDS, tuberculosis and malaria programs: estimation approach and results between 2003 and end-2007. BMC Infect Dis 2010;10:109. - PMC - PubMed
-
- World Health Organization. Global tuberculosis control: WHO report 2011. Geneva: WHO Press; 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
