

Blood pressure excursions below the cerebral autoregulation threshold during cardiac surgery are associated with acute kidney injury
- PMID: 23263580
- PMCID: PMC3769417
- DOI: 10.1097/CCM.0b013e31826ab3a1
Blood pressure excursions below the cerebral autoregulation threshold during cardiac surgery are associated with acute kidney injury
Abstract
Objectives: To determine whether mean arterial blood pressure excursions below the lower limit of cerebral blood flow autoregulation during cardiopulmonary bypass are associated with acute kidney injury after surgery.
Setting: Tertiary care medical center.
Patients: Four hundred ten patients undergoing cardiac surgery with cardiopulmonary bypass.
Design: Prospective observational study.
Interventions: None.
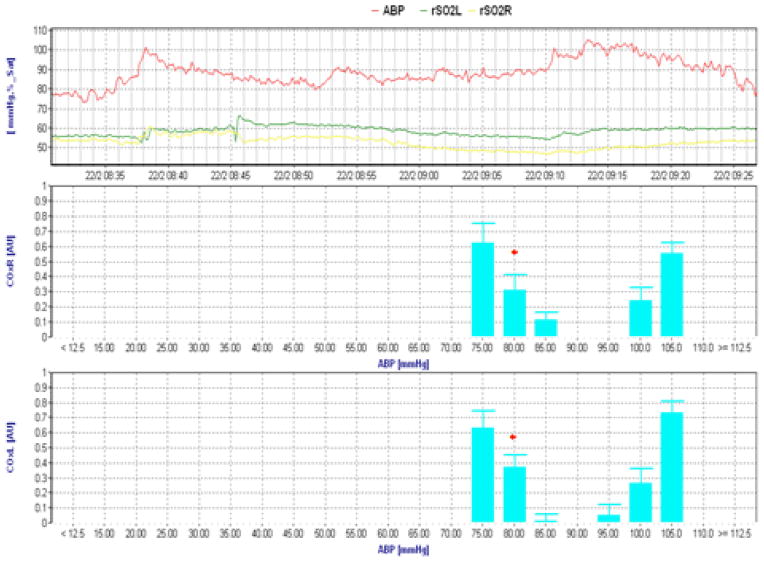
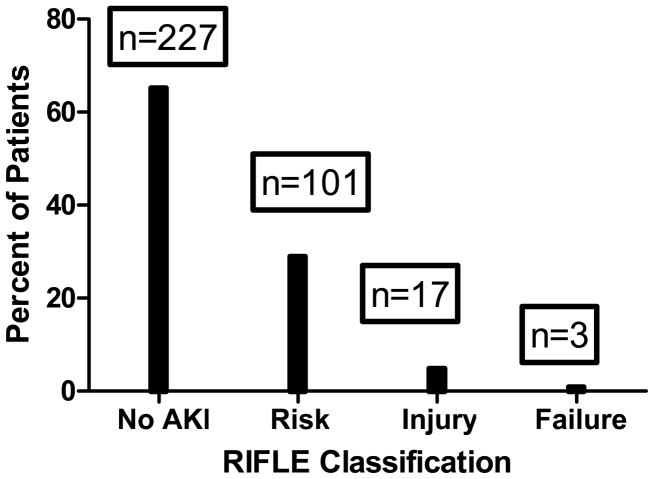
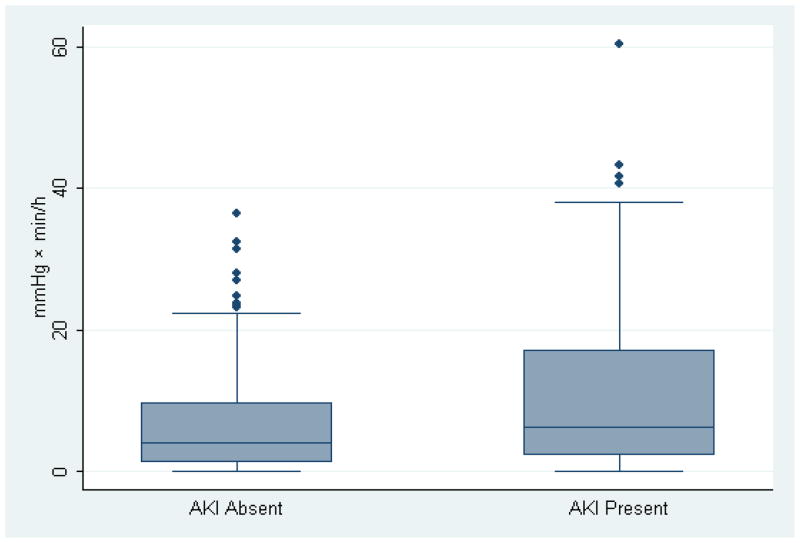
Measurements and main results: Autoregulation was monitored during cardiopulmonary bypass by calculating a continuous, moving Pearson's correlation coefficient between mean arterial blood pressure and processed near-infrared spectroscopy signals to generate the variable cerebral oximetry index. When mean arterial blood pressure is below the lower limit of autoregulation, cerebral oximetry index approaches 1, because cerebral blood flow is pressure passive. An identifiable lower limit of autoregulation was ascertained in 348 patients. Based on the RIFLE criteria (Risk, Injury, Failure, Loss of kidney function, End-stage renal disease), acute kidney injury developed within 7 days of surgery in 121 (34.8%) of these patients. Although the average mean arterial blood pressure during cardiopulmonary bypass did not differ, the mean arterial blood pressure at the limit of autoregulation and the duration and degree to which mean arterial blood pressure was below the autoregulation threshold (mm Hg × min/hr of cardiopulmonary bypass) were both higher in patients with acute kidney injury than in those without acute kidney injury. Excursions of mean arterial blood pressure below the lower limit of autoregulation (relative risk 1.02; 95% confidence interval 1.01 to 1.03; p < 0.0001) and diabetes (relative risk 1.78; 95% confidence interval 1.27 to 2.50; p = 0.001) were independently associated with for acute kidney injury.
Conclusions: Excursions of mean arterial blood pressure below the limit of autoregulation and not absolute mean arterial blood pressure are independently associated with for acute kidney injury. Monitoring cerebral oximetry index may provide a novel method for precisely guiding mean arterial blood pressure targets during cardiopulmonary bypass.
Figures
Comment in
-
Monitoring the brain to save the kidneys.Crit Care Med. 2013 Feb;41(2):671-2. doi: 10.1097/CCM.0b013e318274247e. Crit Care Med. 2013. PMID: 23353951 No abstract available.
References
-
- Brown JR, Cochran RP, MacKenzie TA, et al. Long-term survival after cardiac surgery is predicted by estimated glomerular filtration rate. Ann Thorac Surg. 2008;86(1):4–11. - PubMed
-
- Karkouti K, Wijeysundera DN, Yau TM, et al. Acute kidney injury after cardiac surgery: focus on modifiable risk factors. Circulation. 2009;119(4):495–502. - PubMed
-
- Kuitunen A, Vento A, Suojaranta-Ylinen R, et al. Acute renal failure after cardiac surgery: evaluation of the RIFLE classification. Ann Thorac Surg. 2006;81(2):542–546. - PubMed
-
- Aronson S, Dyke CM, Stierer KA, et al. The ECLIPSE trials: comparative studies of clevidipine to nitroglycerin, sodium nitroprusside, and nicardipine for acute hypertension treatment in cardiac surgery patients. Anesth Analg. 2008;107(4):1110–1121. - PubMed
-
- Weir MR, Aronson S, Avery EG, et al. Acute kidney injury following cardiac surgery: role of perioperative blood pressure control. Am J Nephrol. 2011;33(5):438–452. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
