

Successful treatment of massive intractable pericardial effusion in a patient with systemic lupus erythematosus with tocilizumab
- PMID: 23264273
- PMCID: PMC4544961
- DOI: 10.1136/bcr-2012-007834
Successful treatment of massive intractable pericardial effusion in a patient with systemic lupus erythematosus with tocilizumab
Abstract
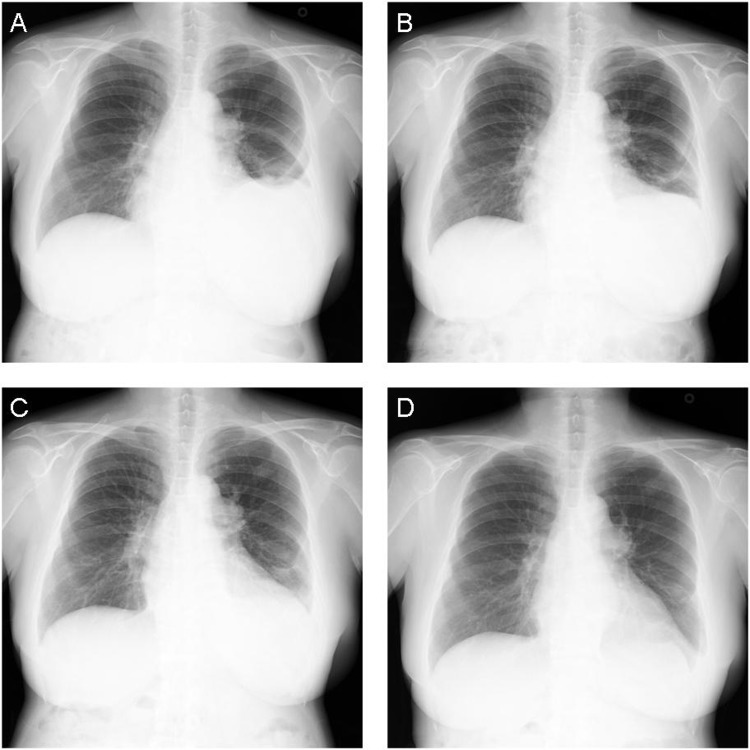
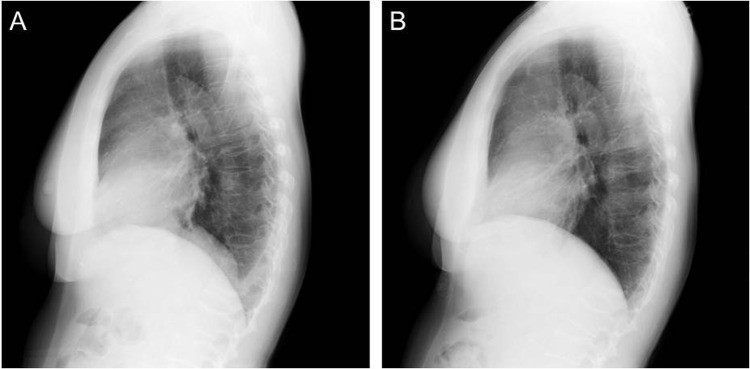
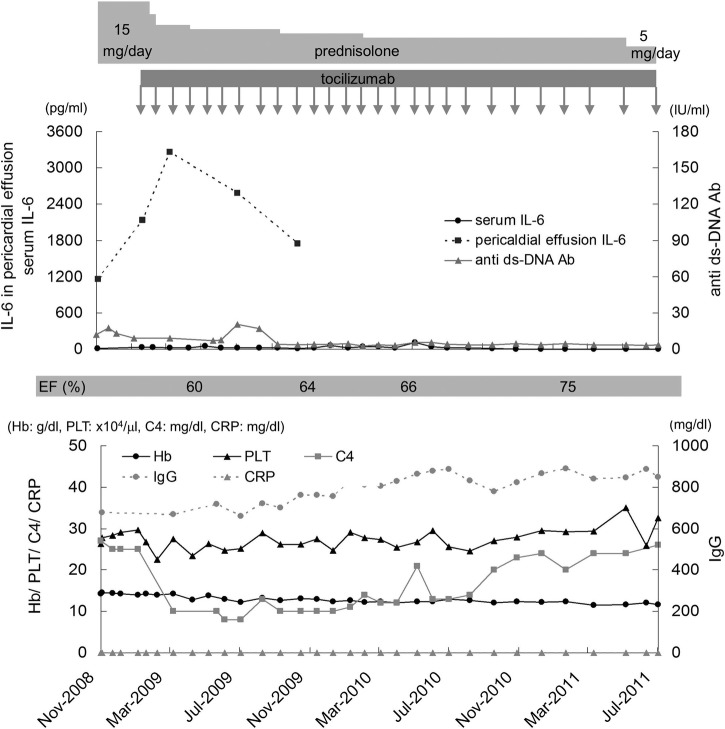
A 51-year-old Japanese woman developed systemic lupus erythematosus (SLE) in 1995. In August 2005, she had massive pericardial effusion due to lupus pericarditis, which was compromising her circulation. Methylprednisolone pulse, intravenous cyclophosphamide pulse and pericardiocentesis were all ineffective. The pericardium was cut surgically to create a passage to drain the liquid into the pleural cavity. The procedure was temporarily effective; however, massive liquid accumulated in the pleural cavity within 1 year. Oral tacrolimus and topical betamethasone injection were ineffective. Since the interleukin-6 (IL-6) level in the effusion was markedly increased (1160 pg/ml), tocilizumab was administered intravenously at a dose of 8 mg/kg every 4 weeks. The effect was astonishing and only a residual amount of pericardial effusion remained. Prednisolone was tapered successfully from 15 to 5 mg daily. Tocilizumab is a treatment of choice when we confront an intractable serositis with massive effusion in SLE, if the IL-6 level is high.
Figures

Similar articles
-
Massive intractable pericardial effusion in a patient with systemic lupus erythematosus treated successfully with pericardial fenestration alone.Lupus. 2008 Nov;17(11):1033-5. doi: 10.1177/0961203308089437. Lupus. 2008. PMID: 18852229
-
Successful treatment of recurrent pleural and pericardial effusions with tocilizumab in a patient with systemic lupus erythematous.BMJ Case Rep. 2016 Aug 8;2016:bcr2016215423. doi: 10.1136/bcr-2016-215423. BMJ Case Rep. 2016. PMID: 27503940 Free PMC article.
-
Short-term add-on tocilizumab and intravenous cyclophosphamide exhibited a remission-inducing effect in a patient with systemic lupus erythematosus with refractory multiorgan involvements including massive pericarditis and glomerulonephritis.Mod Rheumatol. 2017 May;27(3):529-532. doi: 10.3109/14397595.2014.990409. Epub 2014 Dec 30. Mod Rheumatol. 2017. PMID: 25437197
-
Pericardial tamponade complicating systemic lupus erythematosus.J Rheumatol. 1989 Mar;16(3):374-7. J Rheumatol. 1989. PMID: 2657049 Review.
-
Calcified constrictive pericarditis resulting in tamponade in a patient with systemic lupus erythematosus.Rheumatol Int. 2021 Mar;41(3):651-670. doi: 10.1007/s00296-020-04747-6. Epub 2020 Nov 18. Rheumatol Int. 2021. PMID: 33206224 Review.
Cited by
-
P2X7 Receptor Expression in Patients With Serositis Related to Systemic Lupus Erythematosus.Front Pharmacol. 2019 Apr 29;10:435. doi: 10.3389/fphar.2019.00435. eCollection 2019. Front Pharmacol. 2019. PMID: 31110478 Free PMC article.
-
Novel Pharmacotherapies for Recurrent Pericarditis: Current Options in 2020.Curr Cardiol Rep. 2020 Jun 19;22(8):59. doi: 10.1007/s11886-020-01308-y. Curr Cardiol Rep. 2020. PMID: 32562029 Free PMC article. Review.
-
Future prospects in biologic therapy for systemic lupus erythematosus.Nat Rev Rheumatol. 2013 Dec;9(12):705-20. doi: 10.1038/nrrheum.2013.136. Epub 2013 Sep 10. Nat Rev Rheumatol. 2013. PMID: 24018550 Review.
-
Short-term efficacy and safety of rituximab therapy in refractory systemic lupus erythematosus: results from the British Isles Lupus Assessment Group Biologics Register.Rheumatology (Oxford). 2018 Mar 1;57(3):470-479. doi: 10.1093/rheumatology/kex395. Rheumatology (Oxford). 2018. PMID: 29216396 Free PMC article.
-
The conundrum of neuropsychiatric systemic lupus erythematosus: Current and novel approaches to diagnosis.Front Neurol. 2023 Mar 21;14:1111769. doi: 10.3389/fneur.2023.1111769. eCollection 2023. Front Neurol. 2023. PMID: 37025200 Free PMC article. Review.
References
-
- Moder KG, Miller TD, Tazelaar HD. Cardiac involvement in systemic lupus erythematosus. Mayo Clin Proc 1999;74:275–84. - PubMed
-
- Castier MB, Albuquerque EM, Menezes ME, et al. Cardiac tamponade in systemic lupus erythematosus. Report of four cases. Arq Bras Cardiol 2000;75:446–8. - PubMed
-
- Kamata Y, Iwamoto M, Aoki Y, et al. Massive intractable pericardial effusion in a patient with systemic lupus erythematosus treated successfully with pericardial fenestration alone. Lupus 2008;17:1033–5. - PubMed
-
- Sato K, Tsuchiya M, Saldanha J, et al. Reshaping a human antibody to inhibit the interleukin 6-dependent tumor cell growth. Cancer Res 1993;53:851–6. - PubMed
-
- Mihara M, Kasutani K, Okazaki M, et al. Tocilizumab inhibits signal transduction mediated by both mIL-6R and sIL-6R, but not by the receptors of other members of IL-6 cytokine family. Int Immunopharmacol 2005;5:1731–40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical