

Generic and brand-name L-thyroxine are not bioequivalent for children with severe congenital hypothyroidism
- PMID: 23264396
- PMCID: PMC3565118
- DOI: 10.1210/jc.2012-3125
Generic and brand-name L-thyroxine are not bioequivalent for children with severe congenital hypothyroidism
Abstract
Context: In the United States, generic substitution of levothyroxine (L-T(4)) by pharmacists is permitted if the formulations are deemed to be bioequivalent by the Federal Drug Administration, but there is widespread concern that the pharmacokinetic standard used is too insensitive.
Objective: We aimed to evaluate the bioequivalence of a brand-name L-T(4) (Synthroid) and an AB-rated generic formulation (Sandoz, Princeton, NJ) in children with severe hypothyroidism.
Design: This was a prospective randomized crossover study in which patients received 8 weeks of one L-T(4) formulation followed by 8 weeks of the other.
Setting: The setting was an academic medical center.
Patients: Of 31 children with an initial serum TSH concentration >100 mU/L, 20 had congenital hypothyroidism (CH), and 11 had autoimmune thyroiditis.
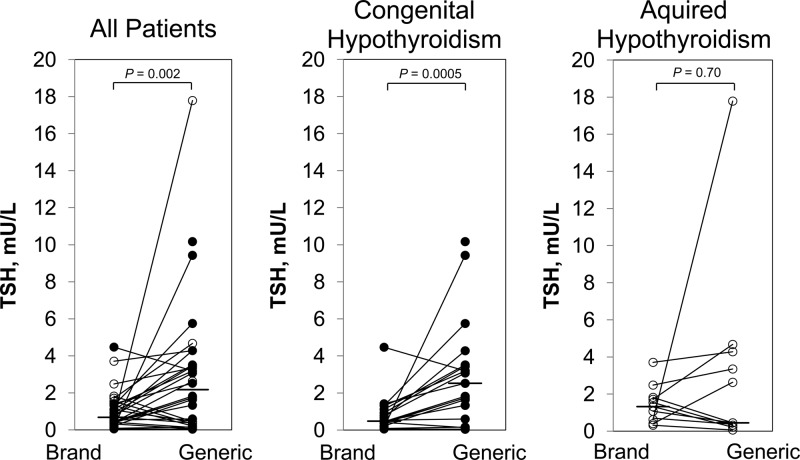
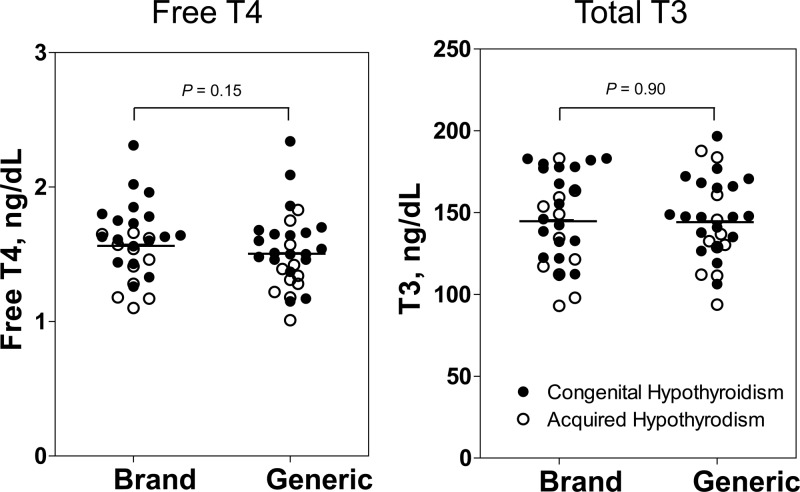
Main outcome measures: The primary endpoint was the serum TSH concentration. Secondary endpoints were the free T(4) and total T(3) concentrations.
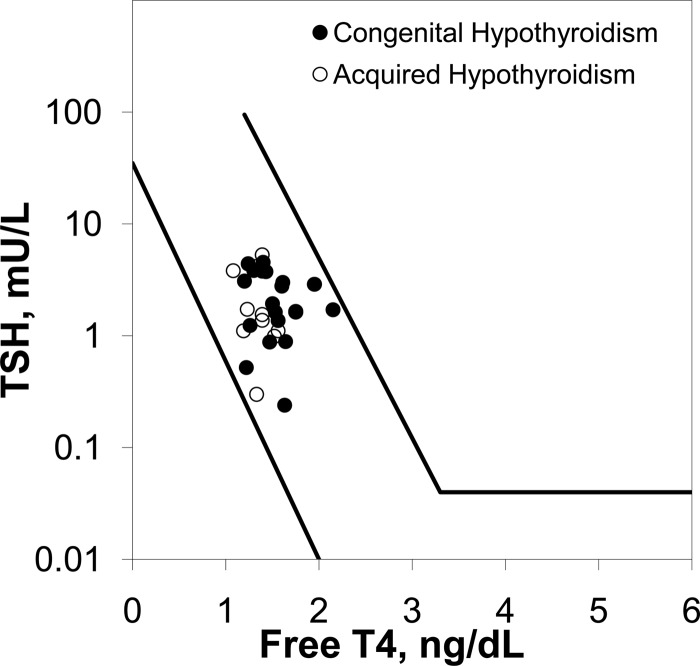
Results: The serum TSH concentration was significantly lower after 8 weeks of Synthroid than after generic drug (P = .002), but thyroid hormone levels did not differ significantly. Subgroup analysis revealed that the difference in TSH was restricted to patients with CH (P = .0005). Patients with CH required a higher L-T(4) dose (P < .0004) and were younger (P = .003) but were not resistant to thyroid hormone; 15 of 16 CH patients had severe thyroid dysgenesis or agenesis on imaging. The response to generic vs brand-name preparation remained significant when adjusted for age.
Conclusions: Synthroid and an AB-rated generic L-T(4) are not bioequivalent for patients with severe hypothyroidism due to CH, probably because of diminished thyroid reserve. It would therefore seem prudent not to substitute L-T(4) formulations in patients with severe CH, particularly in those <3 yr of age. Our results may have important implications for other severely hypothyroid patients in whom precise titration of L-T(4) is necessary.
Figures
Comment in
-
Generic vs name brand L-thyroxine products: interchangeable or still not?J Clin Endocrinol Metab. 2013 Feb;98(2):511-4. doi: 10.1210/jc.2012-4310. J Clin Endocrinol Metab. 2013. PMID: 23390262 No abstract available.
References
-
- Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T4, and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2002;87:489–499 - PubMed
-
- Brown RS. The Thyroid. In: Brook CGD, Clayton PE, Brown RS, eds. Brook's Clinical Pediatric Endocrinology. 6th ed Oxford, UK: Wiley-Blackwell; 2009:250–282
-
- Cooper DS, Biondi B. Subclinical thyroid disease. Lancet. 2012;379:1142–1154 - PubMed
-
- Ross DS, Neer RM, Ridgway EC, Daniels GH. Subclinical hyperthyroidism and reduced bone density as a possible result of prolonged suppression of the pituitary-thyroid axis with l-thyroxine. Am J Med. 1987;82:1167–1170 - PubMed
-
- Jodar E, Begona Lopez M, et al. Bone changes in pre- and postmenopausal women with thyroid cancer on levothyroxine therapy: evolution of axial and appendicular bone mass. Osteoporos Int. 1998;8:311–316 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
