

Evaluating the association of preoperative functional status and postoperative functional decline in older patients undergoing major surgery
- PMID: 23265122
- PMCID: PMC4241019
Evaluating the association of preoperative functional status and postoperative functional decline in older patients undergoing major surgery
Abstract
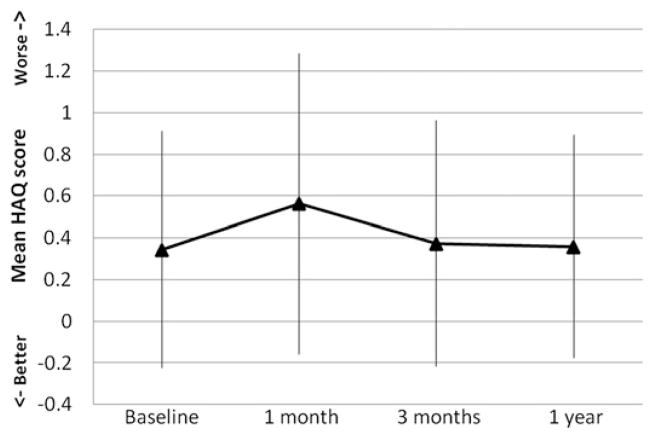
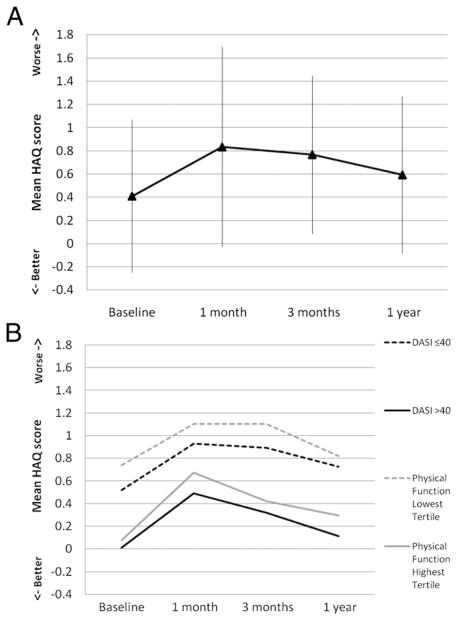
This prospective cohort study sought to identify predictors of functional decline in patients aged 65 years or older who underwent major, nonemergent abdominal or thoracic surgery in our tertiary hospital from 2006 to 2008. We used the Stanford Health Assessment Questionnaire-Disability Index (HAQ-DI) to evaluate functional decline; a 0.1 or greater increase was used to indicate a clinically significant decline. The preoperative Duke Activity Status Index (DASI) and a physical function score (PFS), assessing gait speed, grip strength, balance, and standing speed, were evaluated as predictors of decline. We enrolled 215 patients (71.2 ± 5.2 years; 56.7% female); 204 completed follow-up HAQ assessments (71.1 ± 5.3 years; 57.8% female). A significant number of patients had functional decline out to 1 year. Postoperative HAQ-DI increases of 0.1 or greater occurred in 45.3 per cent at 1 month, 30.1 per cent at 3 months, and 28.3 per cent at 1 year. Preoperative DASI and PFS scores were not predictors of functional decline. Male sex at 1 month (odds ratio [OR], 3.05; 95% confidence interval [CI], 1.41 to 6.85); American Society of Anesthesiologists class (OR, 3.41; 95% CI, 1.31 to 8.86), smoking (OR, 3.15; 95% CI, 1.27 to 7.85), and length of stay (OR, 1.09; 95% CI, 1.01 to 1.16) at 3 months; and cancer diagnosis at 1 year (OR, 2.6; 95% CI, 1.14 to 5.96) were associated with functional decline.
Figures
References
-
- National Center for Health Statistics, Centers for Disease Control and Prevention. [Accessed November 11, 2010]; Available at: www.cdc.gov/nchs.
-
- Thomas DR, Ritchie CS. Preoperative assessment of older adults. J Am Geriatr Soc. 1995;43:811–21. - PubMed
-
- Stamou SC, Dangas G, Dullum MK, et al. Beating heart surgery in octogenarians: perioperative outcome and comparison with younger age groups. Ann Thorac Surg. 2000;69:1140–5. - PubMed
-
- Kirchhoff P, Dincler S, Buchmann P. A multivariate analysis of potential risk factors for intra- and postoperative complications in 1316 elective laparoscopic colorectal procedures. Ann Surg. 2008;248:259–65. - PubMed
-
- Finlayson EV, Birkmeyer JD. Operative mortality with elective surgery in older adults. Eff Clin Pract. 2001;4:172–7. - PubMed