

Review
doi: 10.1179/2047773212Y.0000000047.
Neurocysticercosis in sub-Saharan Africa: a review of prevalence, clinical characteristics, diagnosis, and management
Affiliations
- PMID: 23265550
- PMCID: PMC4005109
- DOI: 10.1179/2047773212Y.0000000047
Item in Clipboard
Review
Neurocysticercosis in sub-Saharan Africa: a review of prevalence, clinical characteristics, diagnosis, and management
Pathog Glob Health.
2012 Sep.
Abstract
Neurocysticercosis has been recognized as a major cause of secondary epilepsy worldwide. So far, most of the knowledge about the disease comes from Latin America and the Indian subcontinent. Unfortunately, in sub-Saharan Africa the condition was neglected for a long time, mainly owing to the lack of appropriate diagnostic tools. This review therefore focuses on the prevalence of neurocysticercosis in sub-Saharan Africa, the clinical picture with emphasis on epilepsy, as well as the diagnosis and treatment of neurocysticercosis and its related epilepsy/epileptic seizures in African resource-poor settings.
Figures
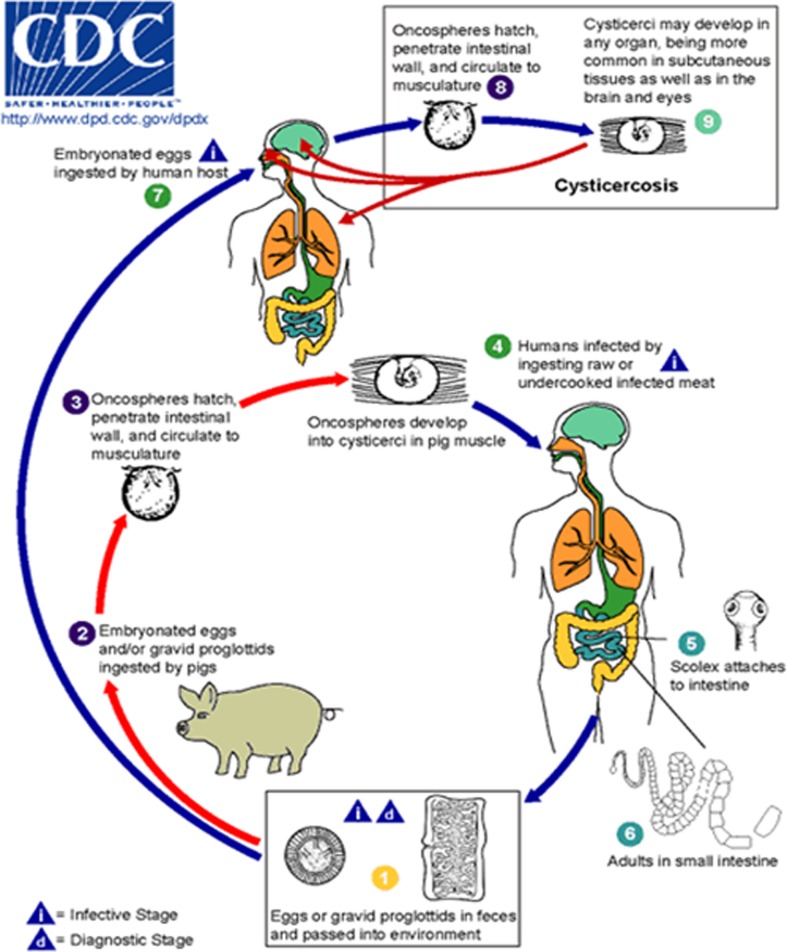
Life cycle of Taenia solium cysticerci. Humans become infected with the adult worm by eating undercooked pork containing cysticerci  and develop taeniosis (tapeworm infection)
and develop taeniosis (tapeworm infection)  ,
,  . Tapeworm eggs or gravid proglottids are excreted from an infected human host into the environment
. Tapeworm eggs or gravid proglottids are excreted from an infected human host into the environment  and can be taken up by freely roaming pigs
and can be taken up by freely roaming pigs  that develop porcine cysticercosis with cysticerci that mainly form in their muscles
that develop porcine cysticercosis with cysticerci that mainly form in their muscles  . The porcine cysticercosis/taeniosis cycle is complete once undercooked infected pork meat is again consumed by a human host
. The porcine cysticercosis/taeniosis cycle is complete once undercooked infected pork meat is again consumed by a human host  . Taenia solium eggs are not only infectious to pigs (paratenic or intermediate hosts) but also to humans
. Taenia solium eggs are not only infectious to pigs (paratenic or intermediate hosts) but also to humans  ,
,  . They can be ingested following direct or indirect (via faecal matter) contact with tapeworm carriers
. They can be ingested following direct or indirect (via faecal matter) contact with tapeworm carriers  ,
,  , which represents the most common route of infection, as well as through the consumption of water or food contaminated with tapeworm eggs
, which represents the most common route of infection, as well as through the consumption of water or food contaminated with tapeworm eggs  . However, the latter is of much less relevance. When humans ingest Taenia solium eggs
. However, the latter is of much less relevance. When humans ingest Taenia solium eggs  through faecal–oral transmission or possible autoinfection, they become accidental hosts of the larval stage of the parasite and develop human cysticercosis
through faecal–oral transmission or possible autoinfection, they become accidental hosts of the larval stage of the parasite and develop human cysticercosis  . Centers for Disease Control and Prevention’s website for parasite identification:
. Centers for Disease Control and Prevention’s website for parasite identification: http://www.dpd.cdc.gov/dpdx/HTML/Taeniasis.htm .
and develop taeniosis (tapeworm infection) , . Tapeworm eggs or gravid proglottids are excreted from an infected human host into the environment and can be taken up by freely roaming pigs that develop porcine cysticercosis with cysticerci that mainly form in their muscles . The porcine cysticercosis/taeniosis cycle is complete once undercooked infected pork meat is again consumed by a human host . Taenia solium eggs are not only infectious to pigs (paratenic or intermediate hosts) but also to humans , . They can be ingested following direct or indirect (via faecal matter) contact with tapeworm carriers , , which represents the most common route of infection, as well as through the consumption of water or food contaminated with tapeworm eggs . However, the latter is of much less relevance. When humans ingest Taenia solium eggs through faecal–oral transmission or possible autoinfection, they become accidental hosts of the larval stage of the parasite and develop human cysticercosis . Centers for Disease Control and Prevention’s website for parasite identification: 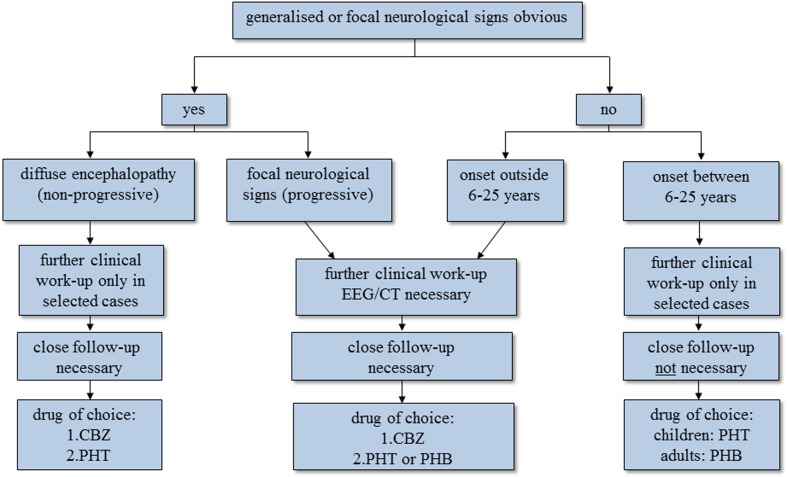
Algorithm on how to classify people with epilepsy/epileptic seizures in resource-poor countries with diagnostic and therapeutic implications. The first question one has to ask is whether there is any evidence of focal neurological signs or even more widespread encephalopathy. If there is, the approach in the two groups is different. In most people, mainly children, with epilepsy with diffuse encephalopathy, diagnostic tests are rarely needed as the extent of the cerebral sequelae is known and the condition is not progressive. In contrast, in people with epilepsy who show focal signs without diffuse encephalopathy further diagnostic steps are essential in order to identify the underlying, potentially treatable cause. If neurological examination is unremarkable, the so-called primary generalised seizures are split according to the age of onset (see text); the two groups have a different diagnostic and therapeutic approach. Patients with primary generalised seizures that start outside 6–25 years are more likely to have cerebral lesions compared to those with seizures that start within the range of 6–25 years, where genetically determined epilepsy prevails. The former therefore need further investigation. In all four groups, treatment depends mainly on the age of the patient, seizure activity, seizure frequency, the presence of mental handicap and the presence of focal neurological signs, bearing in mind that the choice of antiepileptic medication is limited. People with epilepsy/epileptic seizures due to NCC can potentially be found in all four groups, but are mainly seen in patients with generalised late-onset seizures or in patients with generalised seizures and focal neurological signs without major encephalopathy. For further explanations refer to the main text. CBZ = carbamazepine, PHT = phenytoin, PHB = phenobarbitone.
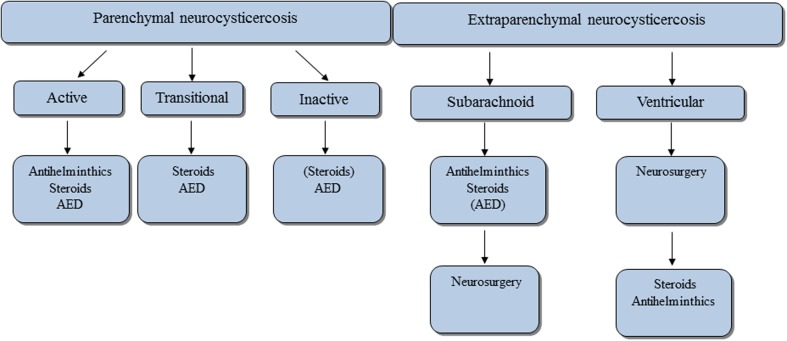
Overview on treatment of NCC according to current guidelines., Treatment approach in people with NCC is divided into those with intraparenchymal and those with extraparenchymal disease. According to disease stage and localisation of lesions different approaches are advocated. Antihelminthic drugs are only administered in active disease. If there are signs of cerebral oedema steroids are used with and without antihelminthic medication. Steroids are also used prophylactically together with antihelminthic medication in active disease without cerebral oedema, as oedema may develop over the course of treatment. In multicystic disease with obvious oedema ( = encephalitis) antihelminthic medication must not be used and the treatment of choice are steroids alone or in combination with antiepileptic medication. The latter is used in all stages whenever epileptic seizures are present. In subarachnoid disease antihelminthic medication together with steroids may have to be given in higher doses and over longer time than in patients with intraparenchymal disease. The same is true for ventricular disease, although the first line treatment is surgery with removal of the ventricular cysts. AED = antiepileptic medication.
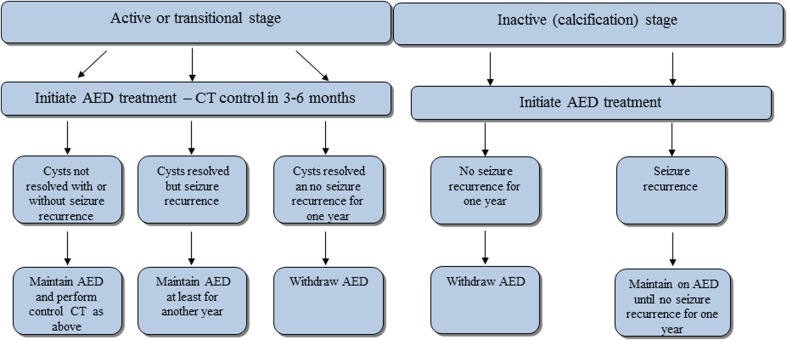
Withdrawal algorithm of antiepileptic medication in people with epilepsy due to NCC. If CT is at hand, we suggest following the indicated algorithm which refers to people with NCC of various disease stages who previously have been put on antiepileptic medication. In a nutshell, withdrawal is guided by the presence or absence of intracerebral lesions and by seizure recurrence. We have defined seizure recurrence as at least one seizure during the last year as this seems to be the accepted time frame for initiation of antiepileptic treatment in resource-poor settings. For more details refer to the main text. AED = antiepileptic medication, CT = computed tomography. Adapted from Carpio 2012: http://emedicine.medscape.com/article/1168784-overview#a0199 .
References
-
- Preux PM, Druet-Cabanac M. Epidemiology and aetiology of epilepsy in sub-Saharan Africa. Lancet Neurol. 2005;4:21–31. - PubMed
-
- Del Brutto OH.Helminthic infections of the central nervous system Noseworthy J H, ed, editor. Neurological therapeutic principles and practice. 2nd edAbingdon, Oxon: Informa Health Care; 2006. p. 1133–52.
-
- Campbell CD, Farrell VJR. Brain scans, epilepsy and cerebral cysticercosis. S Afr Med J. 1987;72:885–6. - PubMed
-
- Carpio A, Hauser WA. Prognosis for seizure recurrence in patients with newly diagnosed neurocysticercosis. Neurology. 2002;59:1730–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical