

Differential outcomes of carotid stenting and endarterectomy performed exclusively by vascular surgeons in the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST)
- PMID: 23265585
- PMCID: PMC3645486
- DOI: 10.1016/j.jvs.2012.09.014
Differential outcomes of carotid stenting and endarterectomy performed exclusively by vascular surgeons in the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST)
Abstract
Objective: Outcomes in the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST) did not differ between carotid artery stenting (CAS) and carotid endarterectomy (CEA) for the composite primary end point of stroke, myocardial infarction (MI), or death during the periprocedural period or ipsilateral stroke within 4 years. Rigorous credentialing and training of interventionists, including vascular surgeons, were required for the randomization phase of CREST. Because the lead-in phase of CREST had suggested higher perioperative risks after CAS performed by vascular surgeons, the purpose of this analysis was to examine differences in outcomes after randomization between CAS and CEA performed by vascular surgeons.
Methods: CREST is a prospective randomized controlled trial with blinded end point adjudication. Vascular surgeons performed 237 (21%) of the CAS procedures and 765 (65%) of the CEA procedures among 2320 patients who received their assigned treatment. Proportional hazards analyses were used to estimate the relative efficacy of CAS vs CEA for the composite primary end point and also for stroke and death.
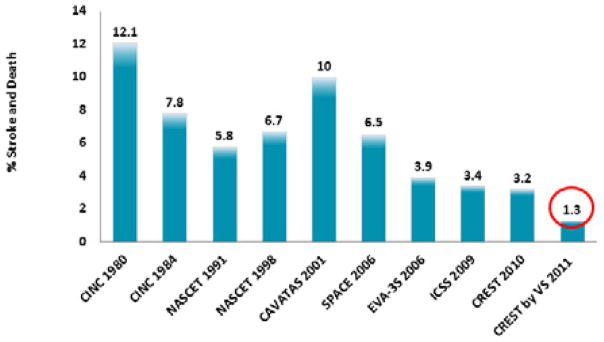
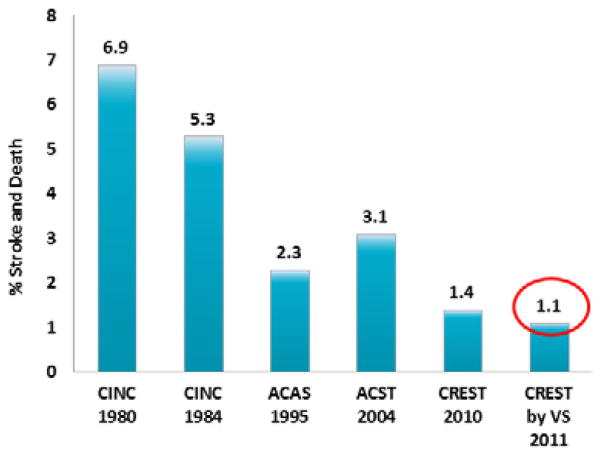
Results: Among 2502 randomized patients, 1321 (53%) were symptomatic and 1181 (47%) were asymptomatic. For procedures performed exclusively by vascular surgeons, the primary end point did not differ between CAS and CEA at 4-year follow-up (6.2% vs 5.6%, respectively; hazard ratio [HR], 1.30; 95% confidence interval [CI], 0.70-2.41; P = .41) In this subgroup, the periprocedural stroke and death rates were higher after CAS than CEA for symptomatic patients (6.1% vs 1.3%; P = .01). Asymptomatic patients also had slightly higher stroke and death rates after CAS (2.6% vs 1.1%; P = .20), although this difference did not reach statistical significance. Conversely, cranial nerve injuries (0.0% vs 5.0%; P < .001) were less frequent after CAS than CEA. The MI rates were slightly lower after CAS (1.3% vs 2.6%; P = .24). In performing CAS, vascular surgeons had outcomes for the periprocedural primary end point comparable to the outcomes of all interventionists (HR, 0.99; 95% CI, 0.50-2.00) after adjusting for age, sex, and symptomatic status. Vascular surgeons also had similar results after CEA for the periprocedural primary end point compared with other surgeons (HR, 0.73; 95% CI, 0.42-1.27).
Conclusions: When performed by surgeons, CAS and CEA have similar net outcomes, although the periprocedural risks vary (lower stroke with CEA and lower MI with CAS). These data suggest that appropriately trained vascular surgeons may safely offer both CEA and CAS for the prevention of stroke. The remarkably low stroke and death rates after CEA performed by vascular surgeons in CREST, particularly among symptomatic patients, represent the best outcomes ever reported after carotid interventions from a randomized controlled trial. ClinicalTrials.gov identifier: NCT0000473.
Trial registration: ClinicalTrials.gov NCT00004732 NCT00000473 NCT00004732.
Copyright © 2013 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Figures
Similar articles
-
Stenting versus endarterectomy after prior ipsilateral carotid endarterectomy.J Vasc Surg. 2017 Jan;65(1):1-11. doi: 10.1016/j.jvs.2016.07.115. Epub 2016 Oct 1. J Vasc Surg. 2017. PMID: 27707617
-
The Carotid Revascularization Endarterectomy vs. Stenting Trial completes randomization: lessons learned and anticipated results.J Vasc Surg. 2009 Nov;50(5):1224-31. doi: 10.1016/j.jvs.2009.09.003. J Vasc Surg. 2009. PMID: 19878793 Free PMC article. Clinical Trial.
-
Duration of asymptomatic status and outcomes following carotid endarterectomy and carotid artery stenting in the Carotid Revascularization Endarterectomy vs Stenting Trial.J Vasc Surg. 2019 Jun;69(6):1797-1800. doi: 10.1016/j.jvs.2018.09.054. Epub 2019 Jan 8. J Vasc Surg. 2019. PMID: 30630649 Free PMC article. Clinical Trial.
-
Critique of the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST): flaws in CREST and its interpretation.Eur J Vasc Endovasc Surg. 2013 Jun;45(6):539-45. doi: 10.1016/j.ejvs.2013.03.014. Epub 2013 Apr 19. Eur J Vasc Endovasc Surg. 2013. PMID: 23602856 Review.
-
Carotid artery stenting versus carotid endarterectomy: updated meta-analysis, metaregression and trial sequential analysis of short-term and intermediate-to long-term outcomes of randomized trials.J Cardiovasc Surg (Torino). 2016 Aug;57(4):519-39. Epub 2016 Feb 17. J Cardiovasc Surg (Torino). 2016. PMID: 26883249 Review.
Cited by
-
Long-term outcomes of carotid stenting in a single neurovascular center: up to 12-year retrospective analysis with a focus on the influence of comorbidities.Neuroradiology. 2024 Jan;66(1):117-127. doi: 10.1007/s00234-023-03248-0. Epub 2023 Nov 27. Neuroradiology. 2024. PMID: 38010404
-
Decreased ¹³N-labeled ammonia uptake in the ipsilateral and contralateral hemispheres following carotid endarterectomy.Mol Med Rep. 2015 Nov;12(5):6598-604. doi: 10.3892/mmr.2015.4303. Epub 2015 Sep 9. Mol Med Rep. 2015. PMID: 26351875 Free PMC article.
-
Predictors of Perioperative Stroke/Death after Carotid Artery Stenting: A Review Article.Ann Vasc Dis. 2018 Mar 25;11(1):15-24. doi: 10.3400/avd.ra.17-00136. Ann Vasc Dis. 2018. PMID: 29682104 Free PMC article. Review.
-
Cardiac damage after carotid intervention: a meta-analysis after a decade of randomized trials.J Anesth. 2014 Dec;28(6):866-72. doi: 10.1007/s00540-014-1843-5. Epub 2014 May 15. J Anesth. 2014. PMID: 24828849
-
Meta- analysis and meta-regression analysis of the associations between sex and the operative outcomes of carotid endarterectomy.BMC Cardiovasc Disord. 2015 May 9;15:32. doi: 10.1186/s12872-015-0029-x. BMC Cardiovasc Disord. 2015. PMID: 25956903 Free PMC article.
References
-
- Wolf PA, Kannel WB, Gee DL. Epidemiology of strokes in North America. In: Barnett HJM, Stein BM, Mohr JP, Yatsu FM, editors. Stroke: Pathophysiology, Diagnosis and Management. New York: Churchill Livingstone; 1986. pp. 19–29.
-
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991;325:445–53. - PubMed
-
- Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA. 1995;273:1421–8. - PubMed
-
- Moore WS, Barnett HJ, Beebe HG, Bernstein EF, Brener BJ, Brott TG, et al. Guidelines for carotid endarterectomy. A multidisciplinary consensus statement from the Ad Hoc Committee, American Heart Association. Circulation. 1995;91:566–79. - PubMed
-
- Biller J, Feinberg WM, Castaldo JE, Whittemore AD, Harbaugh RE, Dempsey RJ, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation. 1998;97:501–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
