

Sublingual immunotherapy for peanut allergy: a randomized, double-blind, placebo-controlled multicenter trial
- PMID: 23265698
- PMCID: PMC3550002
- DOI: 10.1016/j.jaci.2012.11.011
Sublingual immunotherapy for peanut allergy: a randomized, double-blind, placebo-controlled multicenter trial
Abstract
Background: There are presently no available therapeutic options for patients with peanut allergy.
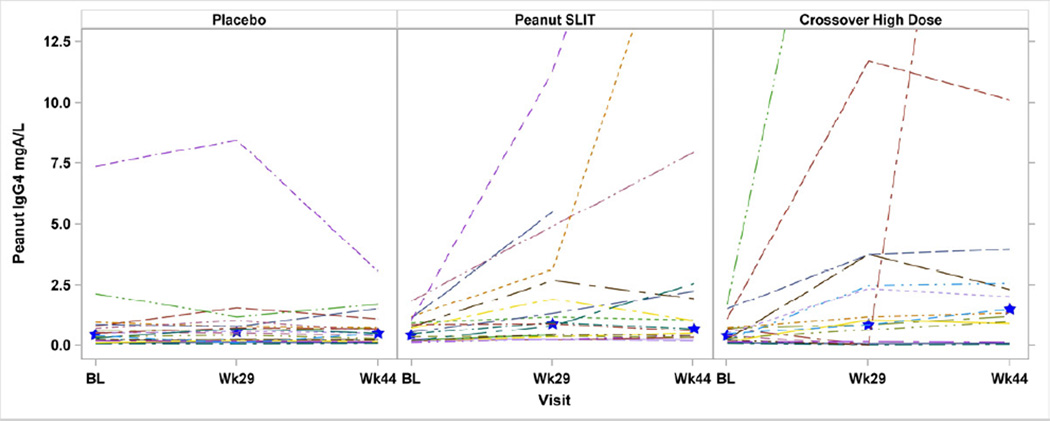
Objective: We sought to investigate the safety, efficacy, and immunologic effects of peanut sublingual immunotherapy (SLIT).
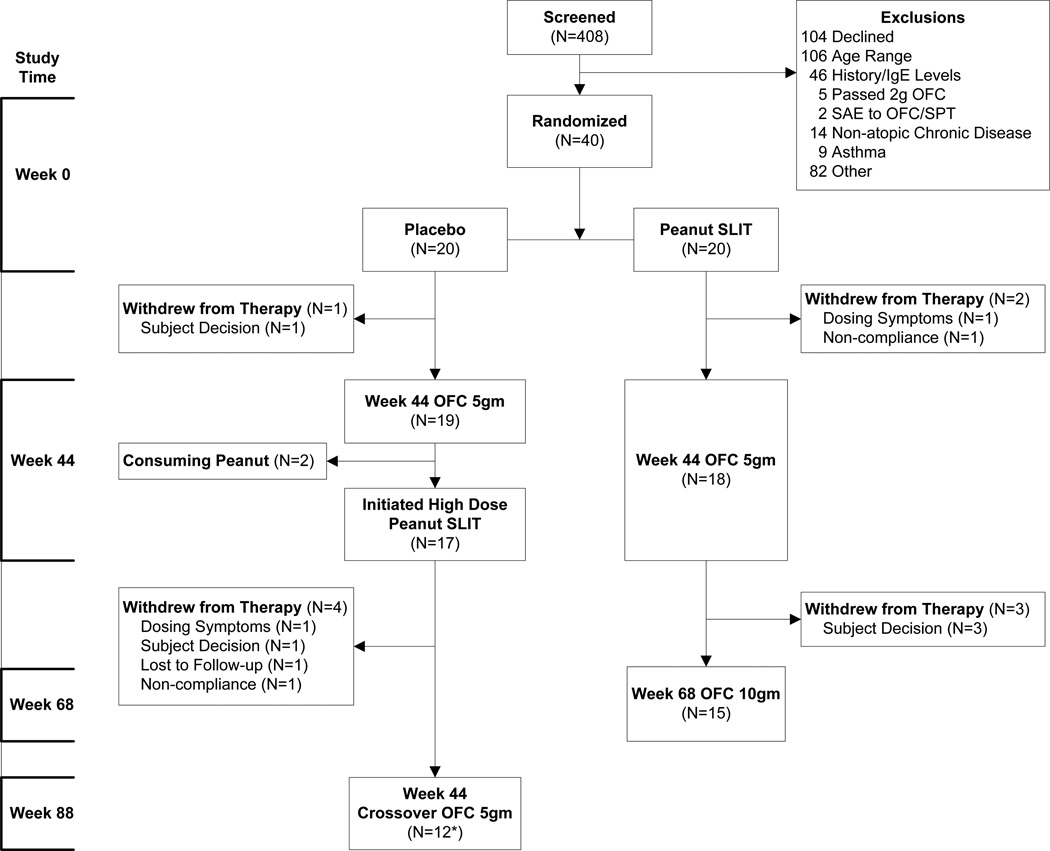
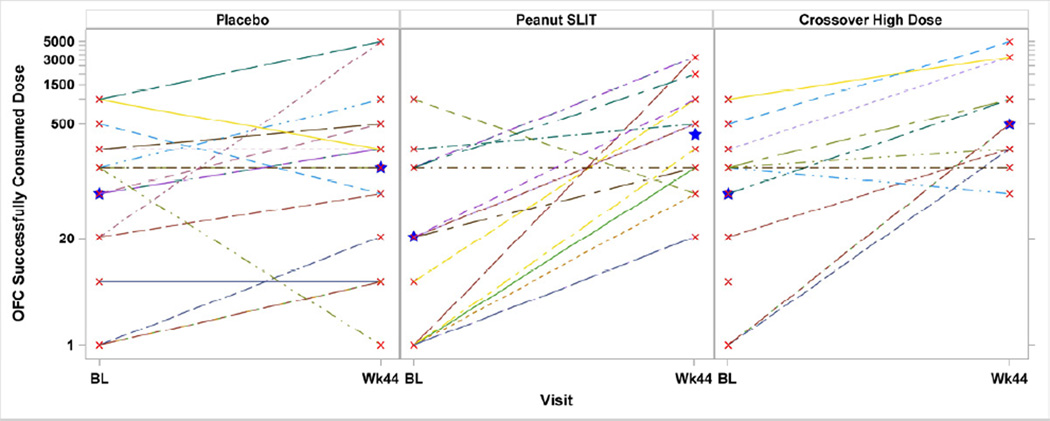
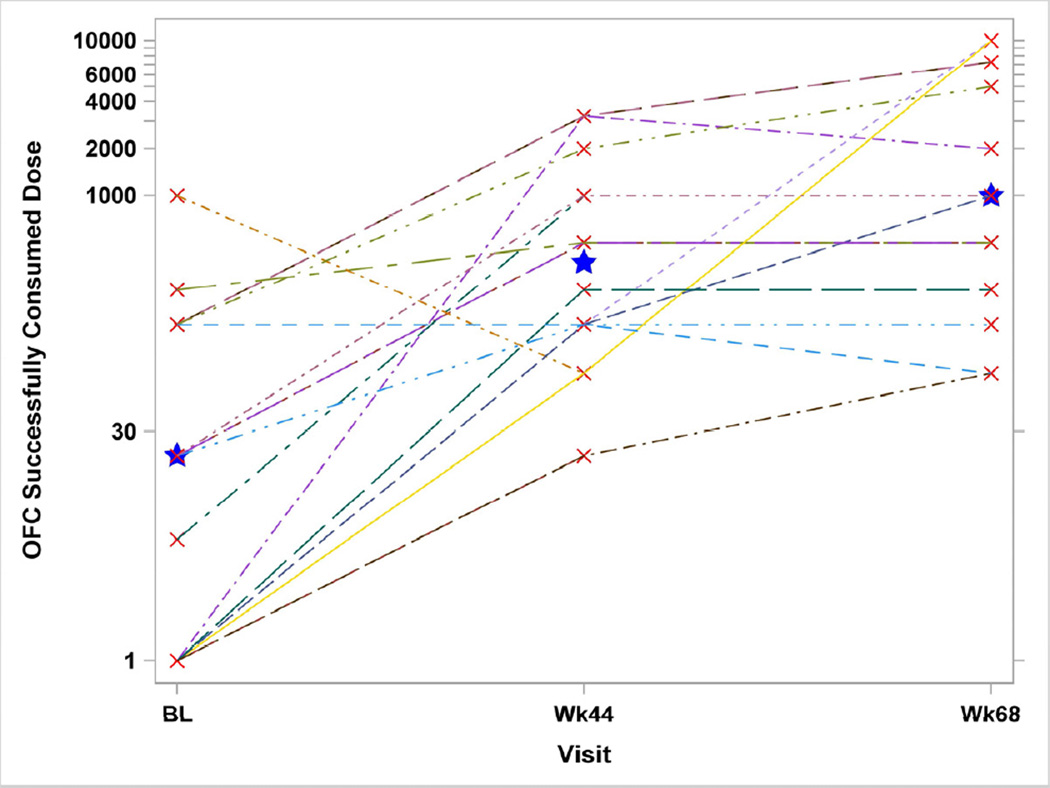
Methods: After a baseline oral food challenge (OFC) of up to 2 g of peanut powder (approximately 50% protein; median successfully consumed dose [SCD], 46 mg), 40 subjects, aged 12 to 37 years (median, 15 years), were randomized 1:1 across 5 sites to daily peanut or placebo SLIT. A 5-g OFC was performed after 44 weeks, followed by unblinding; placebo-treated subjects then crossed over to higher dose peanut SLIT, followed by a subsequent crossover Week 44 5-g OFC. Week 44 OFCs from both groups were compared with baseline OFCs; subjects successfully consuming 5 g or at least 10-fold more peanut powder than the baseline OFC threshold were considered responders.
Results: After 44 weeks of SLIT, 14 (70%) of 20 subjects receiving peanut SLIT were responders compared with 3 (15%) of 20 subjects receiving placebo (P < .001). In peanut SLIT responders, median SCD increased from 3.5 to 496 mg. After 68 weeks of SLIT, median SCD significantly increased to 996 mg (compared with Week 44, P = .05). The median SCD at the Week 44 Crossover OFC was significantly higher than baseline (603 vs 71 mg, P = .02). Seven (44%) of 16 crossover subjects were responders; median SCD increased from 21 to 496 mg among responders. Of 10,855 peanut doses through the Week 44 OFCs, 63.1% were symptom free; excluding oral-pharyngeal symptoms, 95.2% were symptom free.
Conclusions: Peanut SLIT safely induced a modest level of desensitization in a majority of subjects compared with placebo. Longer duration of therapy showed statistically significant increases in the SCD.
Trial registration: ClinicalTrials.gov NCT00580606.
Published by Mosby, Inc.
Figures
References
-
- Sicherer SH, Munoz-Furlong A, Godbold JH, Sampson HA. US prevalence of self reported peanut, tree nut, and sesame allergy: 11-year follow-up. J Allergy Clin Immunol. 2010;125:1322–1326. - PubMed
-
- Bock SA, Munoz-Furlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J Allergy Clin Immunol. 2001;107:191–193. - PubMed
-
- Bock SA, Munoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food: 2001–2006. J Allergy Clin Immunol. 2007;119:1016–1018. - PubMed
-
- Ford LS, Taylor SL, Pacenza R, Niemann LM, Lambrecht DM, Sicherer SH. Food allergen advisory labeling and product contamination with egg, milk, and peanut. J Allergy Clin Immunol. 2010;126:384–385. - PubMed
-
- Sicherer SH, Burks AW, Sampson HA. Clinical Features of Acute Allergic Reactions to Peanut and Tree Nuts in Children. Pediatrics. 1998;102:e6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
