

Intracranial ROSAI-DORFMAN Disease
- PMID: 23267385
- PMCID: PMC3527051
Intracranial ROSAI-DORFMAN Disease
Abstract
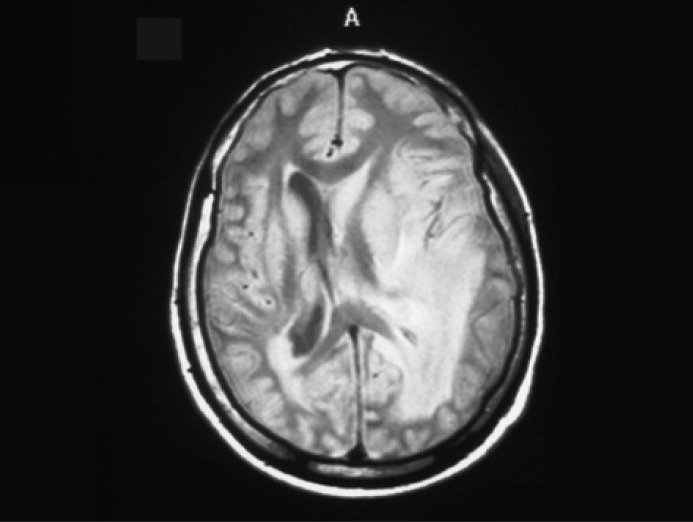
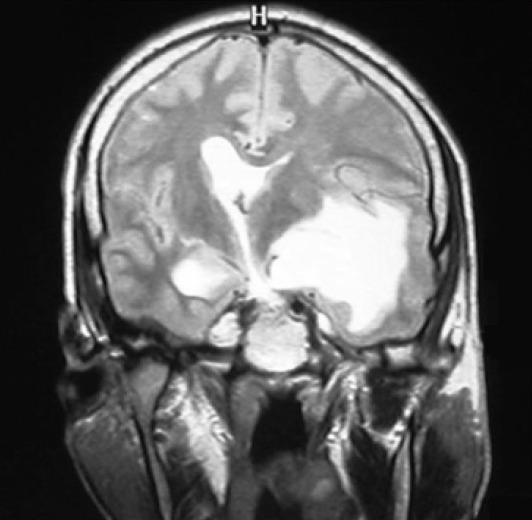
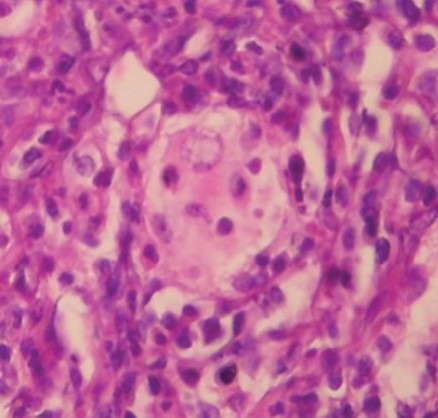
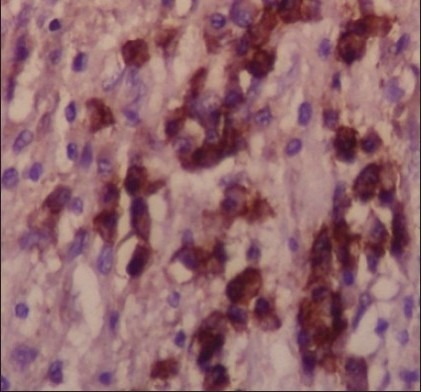
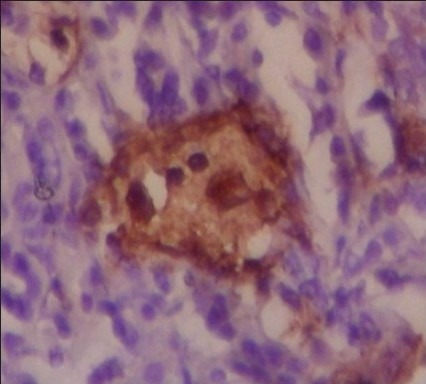
Rosai-Dorfman disease is a benign lymphohistiocytosis that often involve lymph nodes and present as massive lymphadenopathy with sinus histiocytosis. The disease is rarely associated with intracranial involvement. Herein, we report a 33-years-old man with recent onset of unconsciousness. According to his past medical history, he was suffering from frontal headache, ataxia and dizziness with no sensory or motor defect since August 2010. At initial work up, MRI showed infiltrating mass in the left parietal region. Microscopically, the mass consisted of infiltration of abundant lymphoplasma cells, neutrophils and some histiocytes scattered in fibrotic background. Emperipolesis (lymphocytophagocytosis) of histiocytic cells made the diagnosis of Rosai-Dorfman disease. Rosai-Dorfman disease should be added in the list of differential diagnosis for a dural mass mimicking meningioma or cerebral mass mimicking glioma, therefore, immunohistochemical staining for EMA, S100 and CD1a should be performed to rule out the differential diagnosis.
Keywords: Emperipolesis; intracranial Rosai-Dorfman disease.
Conflict of interest statement
Figures
References
-
- Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadeno-pathy: a newly recognized benign clinicopathological entity. Arch Pathol. 1969;87:63–70. - PubMed
-
- Foucar E, Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): Review of the entity. Semin Diagn Pathol. 1990;7:19–73. - PubMed
-
- Fukoshima T, Yachi K, Ogino A, Ohta T, Watanabe T, Yoshino A, et al. Isolated intracranial rosai-Dorfman disease without dural attachment-case report. Neurol Med Chir (Tokyo) 2011;51:136–40. - PubMed
-
- Walid MS, Grigorian AA. Ethmo-spheno-intracranial Rosai-Dorfman disease. Indian J Cancer. 2010;47:80–1. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous