

World allergy organization guidelines for the assessment and management of anaphylaxis
- PMID: 23268454
- PMCID: PMC3500036
- DOI: 10.1097/WOX.0b013e318211496c
World allergy organization guidelines for the assessment and management of anaphylaxis
Abstract
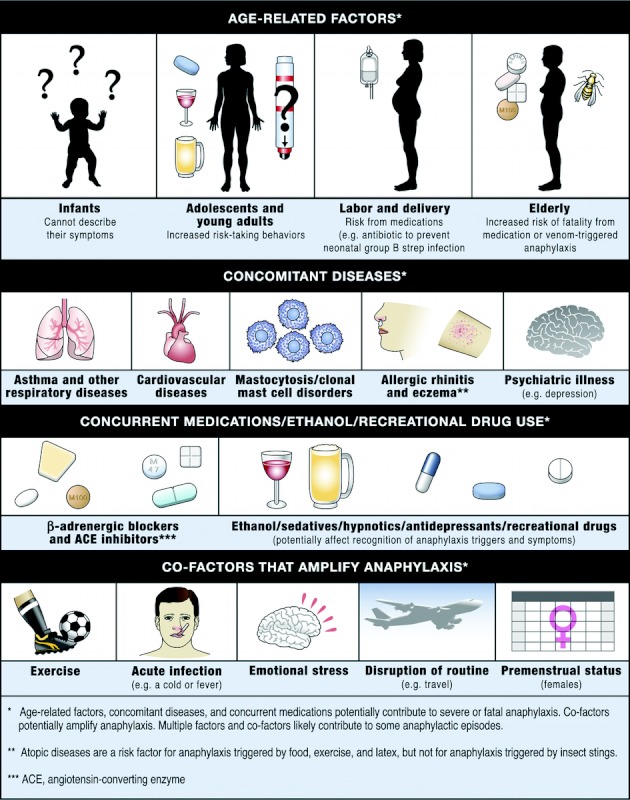
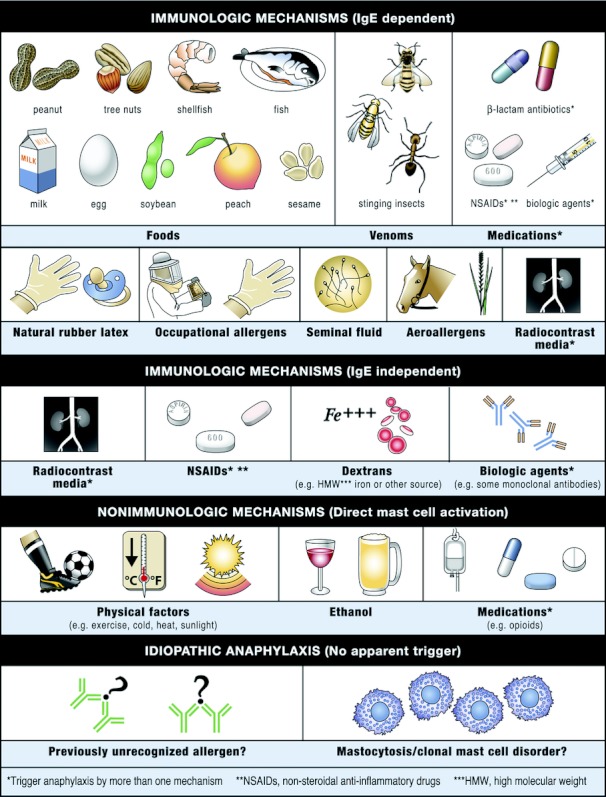
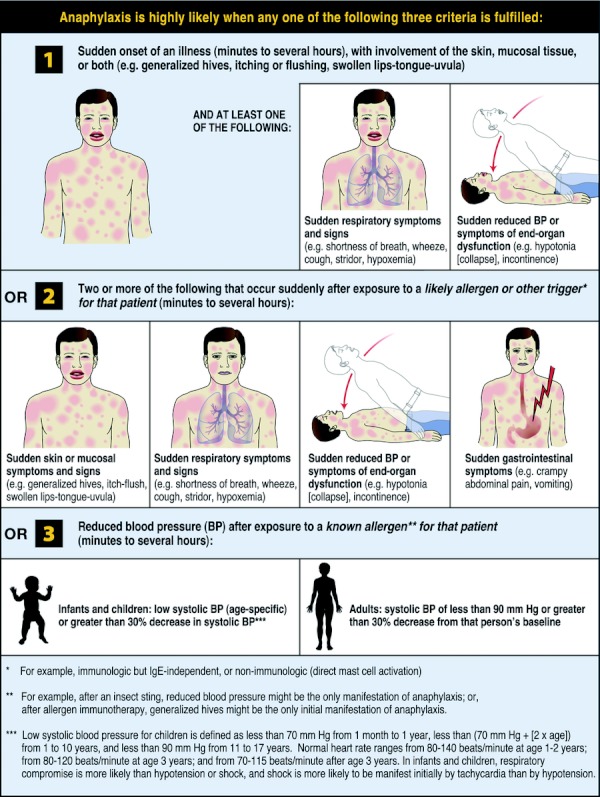
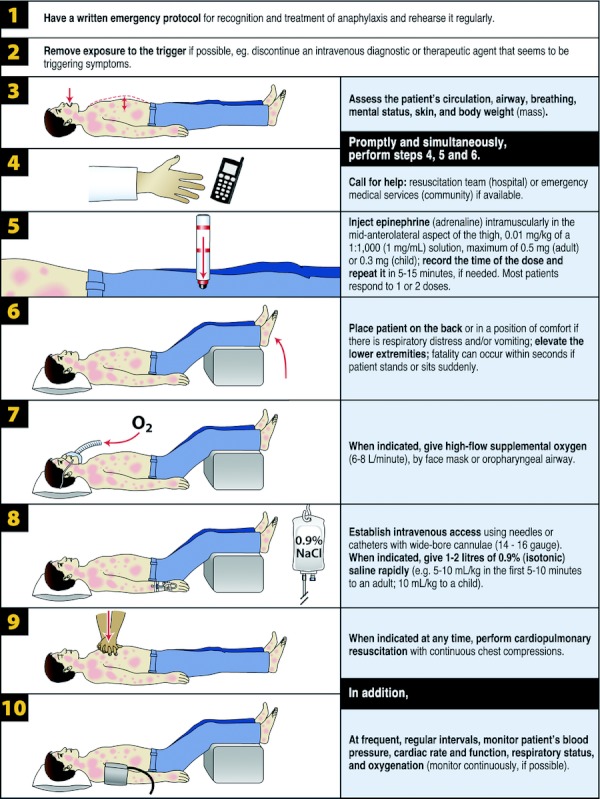
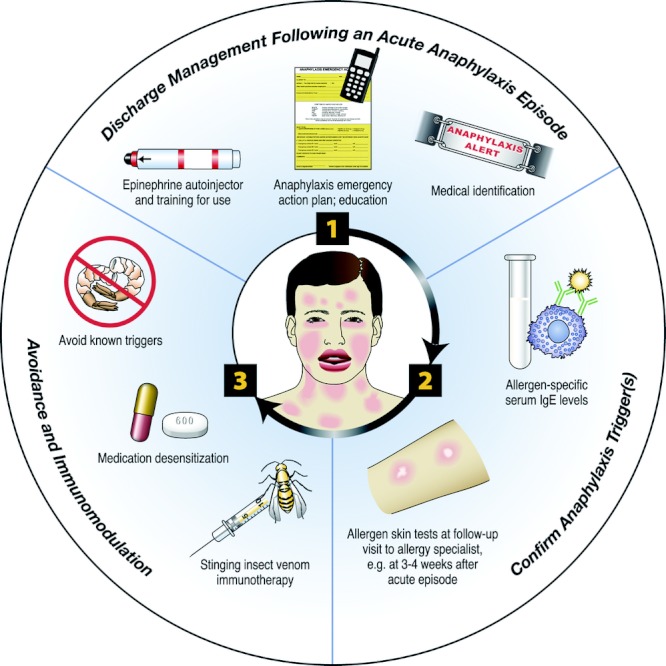
The illustrated World Allergy Organization (WAO) Anaphylaxis Guidelines were created in response to absence of global guidelines for anaphylaxis. Uniquely, before they were developed, lack of worldwide availability of essentials for the diagnosis and treatment of anaphylaxis was documented. They incorporate contributions from more than 100 allergy/immunology specialists on 6 continents. Recommendations are based on the best evidence available, supported by references published to the end of December 2010. The Guidelines review patient risk factors for severe or fatal anaphylaxis, co-factors that amplify anaphylaxis, and anaphylaxis in vulnerable patients, including pregnant women, infants, the elderly, and those with cardiovascular disease. They focus on the supreme importance of making a prompt clinical diagnosis and on the basic initial treatment that is urgently needed and should be possible even in a low resource environment. This involves having a written emergency protocol and rehearsing it regularly; then, as soon as anaphylaxis is diagnosed, promptly and simultaneously calling for help, injecting epinephrine (adrenaline) intramuscularly, and placing the patient on the back or in a position of comfort with the lower extremities elevated. When indicated, additional critically important steps include administering supplemental oxygen and maintaining the airway, establishing intravenous access and giving fluid resuscitation, and initiating cardiopulmonary resuscitation with continuous chest compressions. Vital signs and cardiorespiratory status should be monitored frequently and regularly (preferably, continuously). The Guidelines briefly review management of anaphylaxis refractory to basic initial treatment. They also emphasize preparation of the patient for self-treatment of anaphylaxis recurrences in the community, confirmation of anaphylaxis triggers, and prevention of recurrences through trigger avoidance and immunomodulation. Novel strategies for dissemination and implementation are summarized. A global agenda for anaphylaxis research is proposed.
Figures
References
-
- Johansson SGO, Bieber T, Dahl R, Friedmann PS, Lanier BQ, Lockey RF, et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Allergy Clin Immunol. 2004;113:832–836 - PubMed
-
- Sampson HA, Munoz-Furlong A, Campbell RL, Adkinson NF Jr, Bock SA, Branum A, et al. Second symposium on the definition and management of anaphylaxis: summary report: Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network Symposium. J Allergy Clin Immunol. 2006;117:391–397 - PubMed
-
- Simons FER, for the World Allergy Organization World Allergy Organization survey on global availability of essentials for the assessment and management of anaphylaxis by allergy/immunology specialists in healthcare settings. Ann Allergy Asthma Immunol. 2010;104:405–412 - PubMed
-
- Lieberman P, Camargo CA, Jr, Bohlke K, Jick H, Miller RL, Sheikh A, et al. Epidemiology of anaphylaxis: findings of the American College of Allergy, Asthma and Immunology Epidemiology of Anaphylaxis Working Group. Ann Allergy Asthma Immunol. 2006;97:596–602 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
