

Valid comparisons and decisions based on clinical registers and population based cohort studies: assessing the accuracy, completeness and epidemiological relevance of a breast cancer query database
- PMID: 23270464
- PMCID: PMC3544583
- DOI: 10.1186/1756-0500-5-700
Valid comparisons and decisions based on clinical registers and population based cohort studies: assessing the accuracy, completeness and epidemiological relevance of a breast cancer query database
Abstract
Background: Data accuracy and completeness are crucial for ensuring both the correctness and epidemiological relevance of a given data set. In this study we evaluated a clinical register in the administrative district of Marburg-Biedenkopf, Germany, for these criteria.
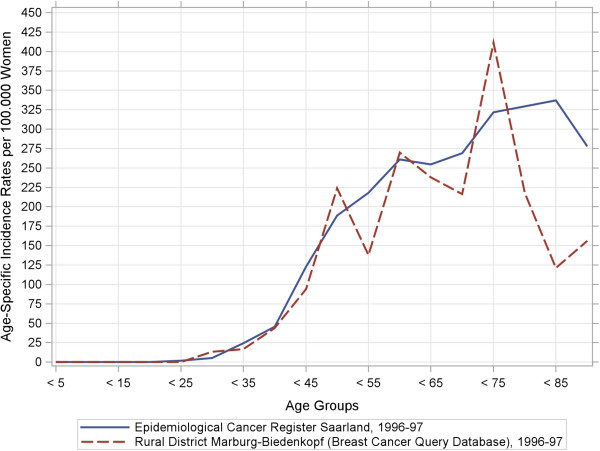
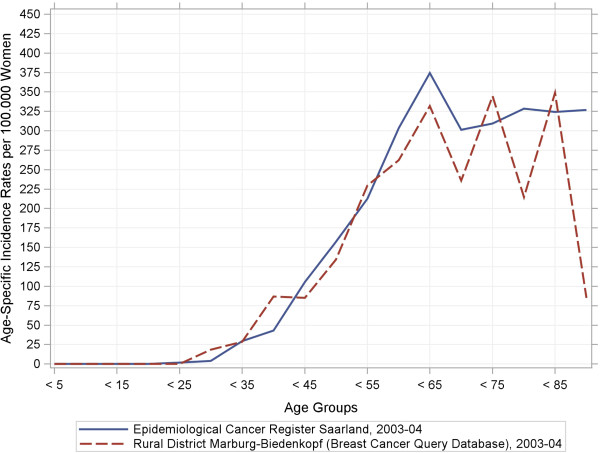
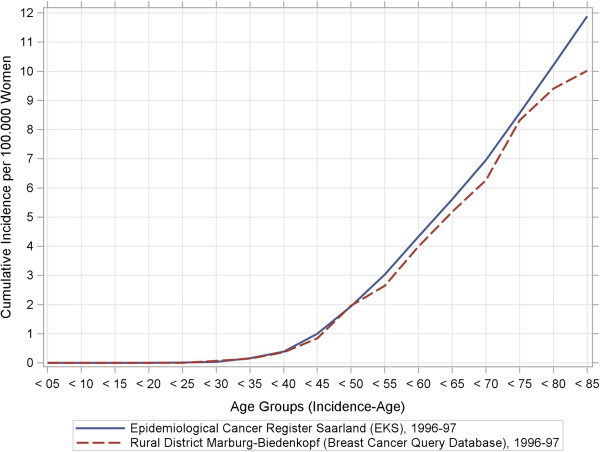
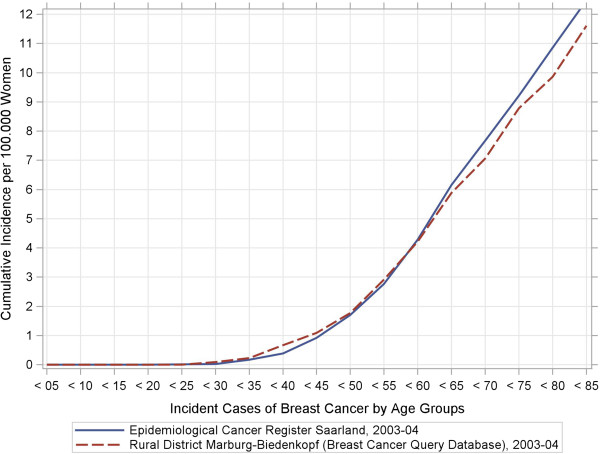
Methods: The register contained data gathered from a comprehensive integrated breast-cancer network from three hospitals that treated all included incident cases of malignant breast cancer in two distinct time periods from 1996-97 (N=389) and 2003-04 (N=488). To assess the accuracy of this data, we compared distributions of risk, prognostic, and predictive factors with distributions from established secondary databases to detect any deviations from these "true" population parameters. To evaluate data completeness, we calculated epidemiological standard measures as well as incidence-mortality-ratios (IMRs).
Results: In total, 12% (13 of 109) of the variables exhibited inaccuracies: 9% (5 out of 56) in 1996-97 and 15% (8 out of 53) in 2003-04. In contrast to raw, unstandardized incidence rates, (in-) directly age-standardized incidence rates showed no systematic deviations. Our final completeness estimates were IMR=36% (1996-97) and IMR=43% (2003-04).
Conclusion: Overall, the register contained accurate, complete, and correct data. Regional differences accounted for detected inaccuracies. Demographic shifts occurred. Age-standardized measures indicate an acceptable degree of completeness. The IMR method of measuring completeness was inappropriate for incidence-based data registers. For the rising number of population-based health-care networks, further methodological advancements are necessary. Correct and epidemiologically relevant data are crucial for clinical and health-policy decision-making.
Figures
References
-
- Sachverständigenrat im Gesundheitswesen (SVRiG) Koordination und Qualität im Gesundheitswesen. Stuttgart: Kohlhammer; 2005.
-
- Sachverständigenrat im Gesundheitswesen (SVRiG) Kooperation und Verantwortung: Voraussetzungen einer zielorientierten Gesundheitsversorgung. Baden-Baden: Nomos; 2007.
-
- Schwartz F, Busse R. In: Das Public Health Buch. Gesundheit fördern - Krankheit verhindern. Schwartz F, Abelin T, Walter U, editor. München: Urban & Fischer; 2003. Denken in Zusammenhängen. Gesundheitssystemforschung; pp. 518–545.
-
- Donabedian A. Evaluating the quality of medical care. The Milbank memorial fund quarterly. 1966;44(Suppl):166–206. - PubMed
-
- Rosner B. Fundamentals of biostatistics. Belmont: Thomson-Brooks/Cole; 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
