

Delirium in the ICU: an overview
- PMID: 23270646
- PMCID: PMC3539890
- DOI: 10.1186/2110-5820-2-49
Delirium in the ICU: an overview
Abstract
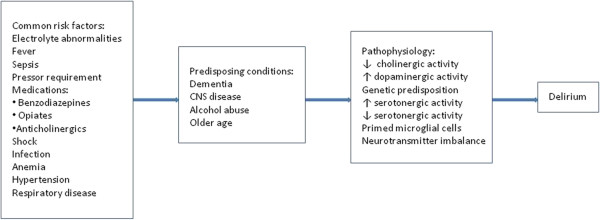
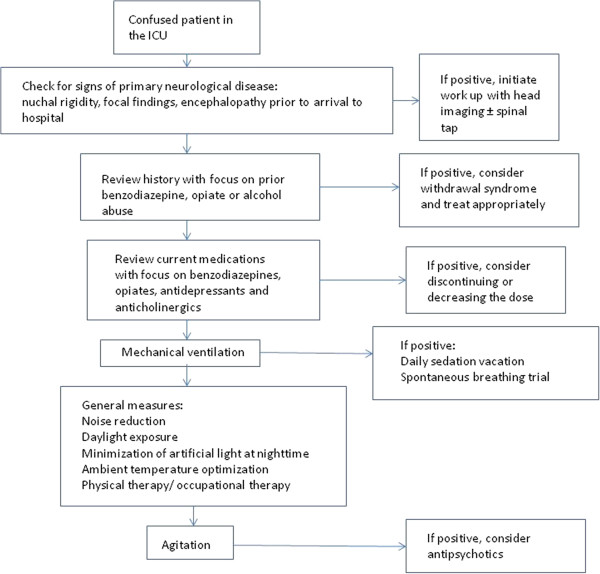
Delirium is characterized by a disturbance of consciousness with accompanying change in cognition. Delirium typically manifests as a constellation of symptoms with an acute onset and a fluctuating course. Delirium is extremely common in the intensive care unit (ICU) especially amongst mechanically ventilated patients. Three subtypes have been recognized: hyperactive, hypoactive, and mixed. Delirium is frequently undiagnosed unless specific diagnostic instruments are used. The CAM-ICU is the most widely studied and validated diagnostic instrument. However, the accuracy of this tool may be less than ideal without adequate training of the providers applying it. The presence of delirium has important prognostic implications; in mechanically ventilated patients it is associated with a 2.5-fold increase in short-term mortality and a 3.2-fold increase in 6-month mortality. Nonpharmacological approaches, such as physical and occupational therapy, decrease the duration of delirium and should be encouraged. Pharmacological treatment for delirium traditionally includes haloperidol; however, more data for haloperidol are needed given the paucity of placebo-controlled trials testing its efficacy to treat delirium in the ICU. Second-generation antipsychotics have emerged as an alternative for the treatment of delirium, and they may have a better safety profile. Dexmedetomidine may prove to be a valuable adjunctive agent for patients with delirium in the ICU.
Figures
References
-
- Anonymous Diagnostic and Statistical Manual of Mental Disorders. 4th. Washington, DC: American Psychiatric Association; 2000.
-
- Salluh JI, Soares M, Teles JM, Ceraso D, Raimondi N, Nava VS, Blasquez P, Ugarte S, Ibanez-Guzman C, Centeno JV, Laca M, Grecco G, Jimenez E, Arias-Rivera S, Duenas C, Rocha MG. Delirium Epidemiology in Critical Care Study Group. Delirium epidemiology in critical care (DECCA): an international study. Crit Care. 2010;14(6):R210. doi: 10.1186/cc9333. - DOI - PMC - PubMed
-
- Agarwal V, O'Neill PJ, Cotton BA, Pun BT, Haney S, Thompson J, Kassebaum N, Shintani A, Guy J, Ely EW, Pandharipande P. Prevalence and risk factors for development of delirium in burn intensive care unit patients. J Burn Care Res. 2010;31(5):706–715. doi: 10.1097/BCR.0b013e3181eebee9. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
