

Predictors of new-onset heart failure: differences in preserved versus reduced ejection fraction
- PMID: 23271790
- PMCID: PMC3705220
- DOI: 10.1161/CIRCHEARTFAILURE.112.972828
Predictors of new-onset heart failure: differences in preserved versus reduced ejection fraction
Abstract
Background: About one half of patients with heart failure (HF) have preserved ejection fraction (HFPEF) rather than reduced ejection fraction (HFREF). The differences in risk factors predisposing to the 2 subtypes of HF are poorly understood. We sought to identify clinical predictors of new-onset HF and to explore differences in HFPEF versus HFREF.
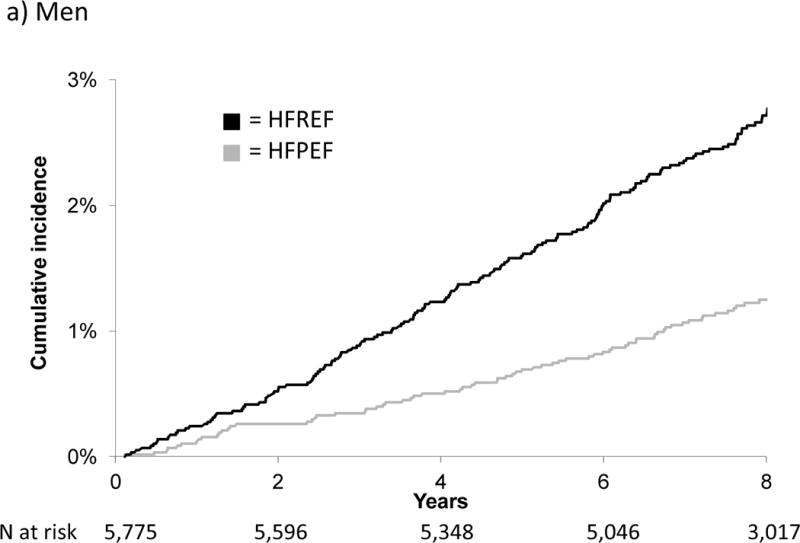
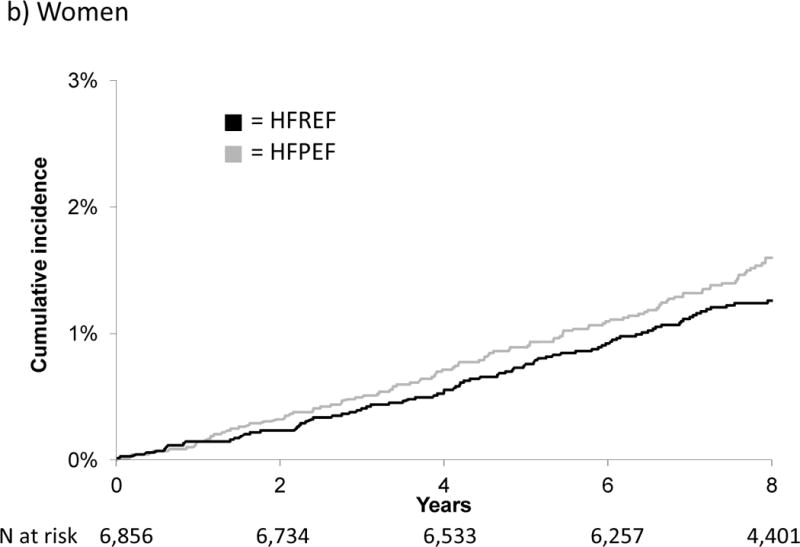
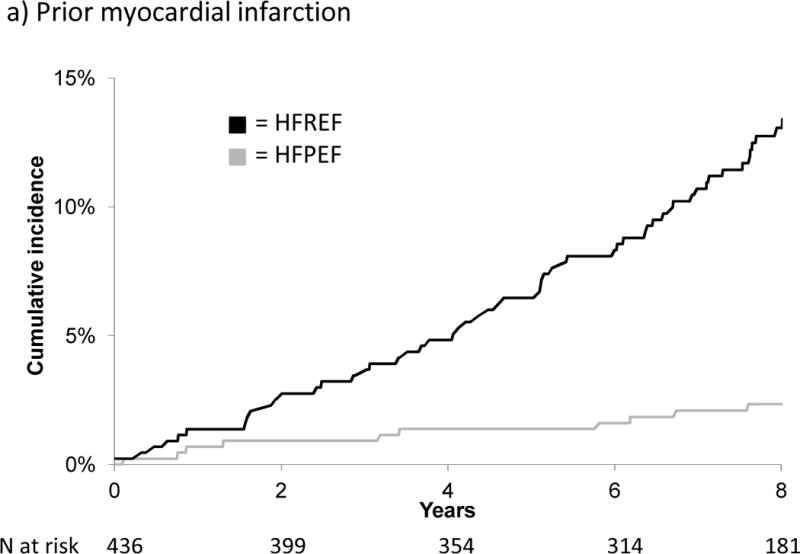
Methods and results: We studied new-onset HF cases between 1981 and 2008 in Framingham Heart Study participants, classified into HFPEF and HFREF (ejection fraction >45% versus ≤45%). We used Cox multivariable regression to examine predictors of 8-year risk of incident HF and competing-risks analysis to identify predictors that differed between HFPEF and HFREF. Among 6340 participants (60±12 years) with 97 808 person-years of follow-up, 512 developed incident HF. Of 457 participants with left ventricular ejection fraction evaluation at the time of HF diagnosis, 196 (43%) were classified as HFPEF and 261 (56%) as HFREF. Fourteen predictors of overall HF were identified. Older age, diabetes mellitus, and a history of valvular disease predicted both types of HF (P≤0.0025 for all). Higher body mass index, smoking, and atrial fibrillation predicted HFPEF only, whereas male sex, higher total cholesterol, higher heart rate, hypertension, cardiovascular disease, left ventricular hypertrophy, and left bundle-branch block predicted risk of HFREF.
Conclusions: Although multiple risk factors preceded overall HF, distinct clusters of risk factors determine risk for new-onset HFPEF versus HFREF. This knowledge may enable the design of clinical trials of targeted prevention and the introduction of therapeutic strategies for prevention of HF and its 2 major subtypes.
Figures

References
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, Ferguson TB, Ford E, Furie K, Gillespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P, Thom T, Wasserthiel-Smoller S, Wong ND, Wylie-Rosett J. Heart disease and stroke statistics--2010 update: A report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- Hogg K, Swedberg K, McMurray J. Heart failure with preserved left ventricular systolic function; epidemiology, clinical characteristics, and prognosis. J Am Coll Cardiol. 2004;43:317–327. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Devereux RB, Roman MJ, Liu JE, Welty TK, Lee ET, Rodeheffer R, Fabsitz RR, Howard BV. Congestive heart failure despite normal left ventricular systolic function in a population-based sample: The Strong Heart Study. Am J Cardiol. 2000;86:1090–1096. - PubMed
-
- Bursi F, Weston SA, Redfield MM, Jacobsen SJ, Pakhomov S, Nkomo VT, Meverden RA, Roger VL. Systolic and diastolic heart failure in the community. JAMA. 2006;296:2209–2216. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
