

Changes in the local tumor microenvironment in recurrent cancers may explain the failure of vaccines after surgery
- PMID: 23271806
- PMCID: PMC3562776
- DOI: 10.1073/pnas.1211850110
Changes in the local tumor microenvironment in recurrent cancers may explain the failure of vaccines after surgery
Abstract
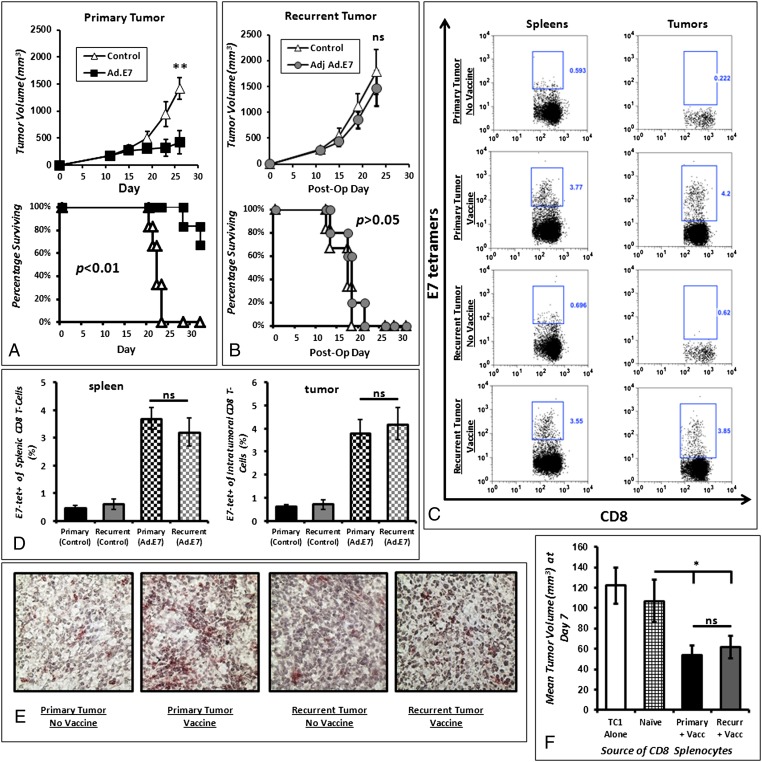
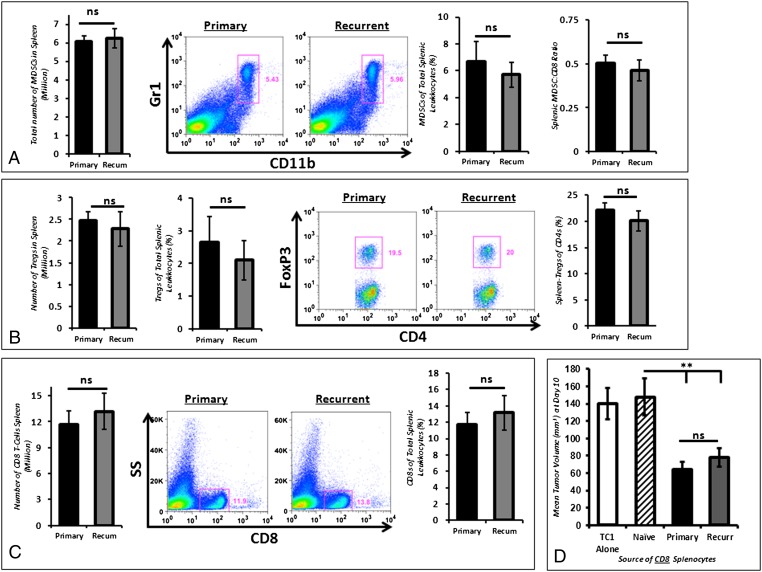
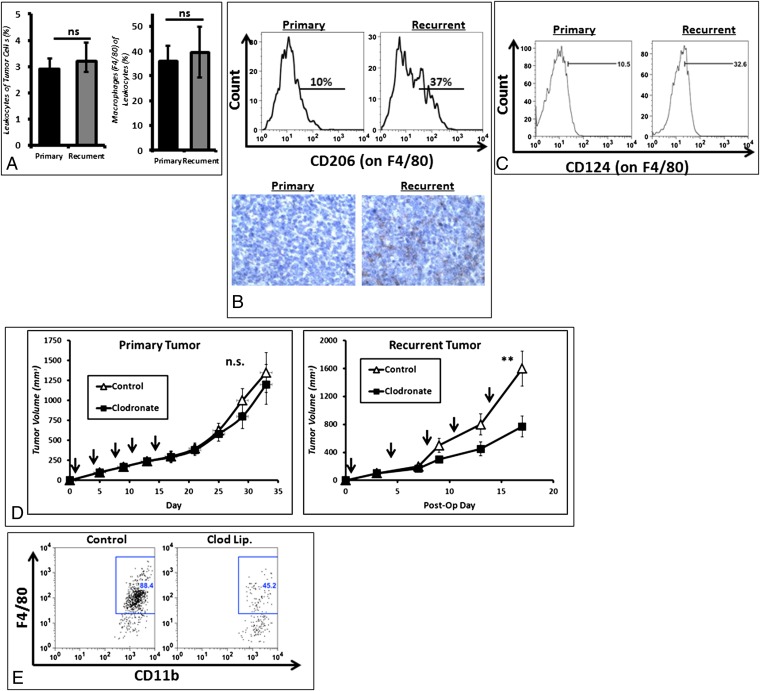
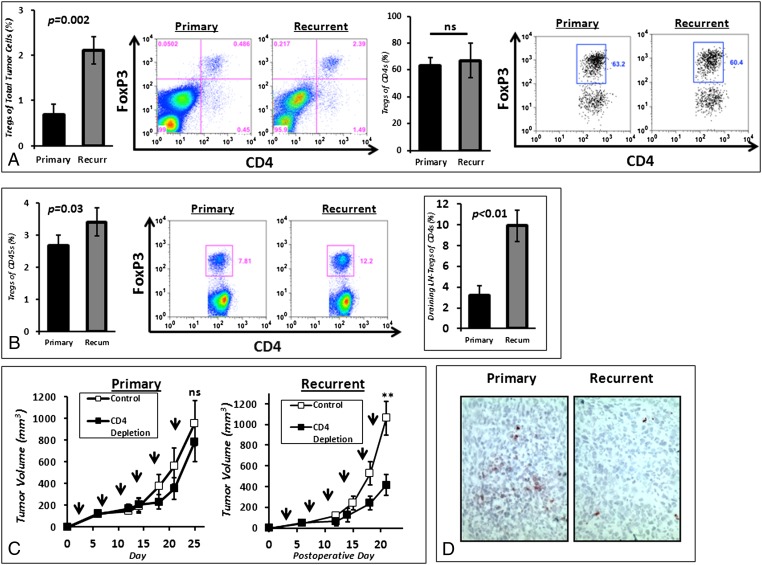
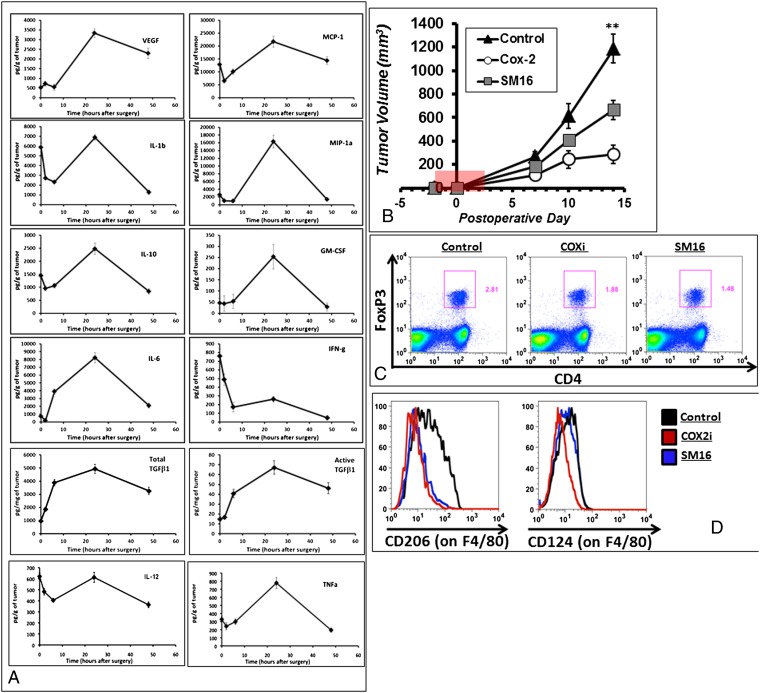
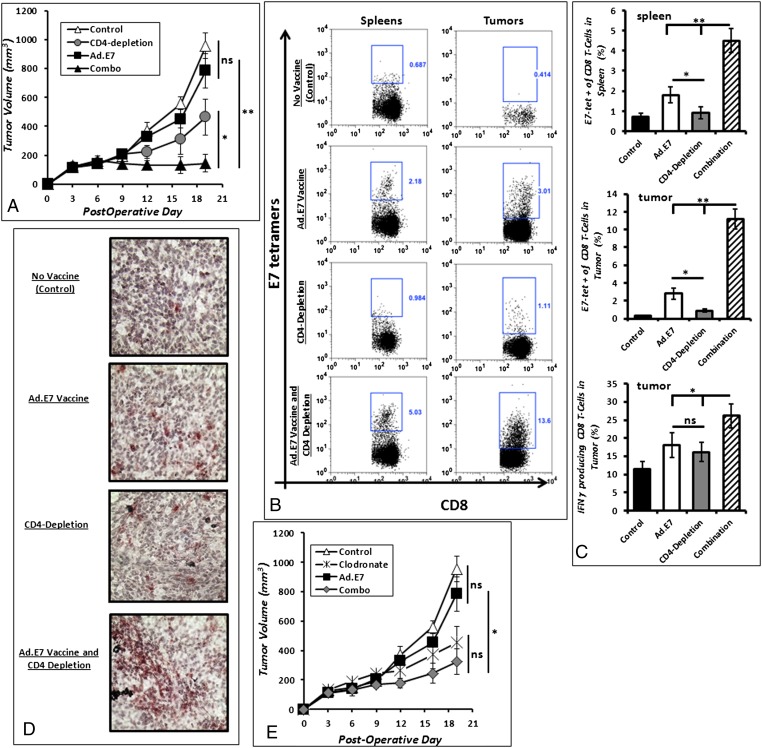
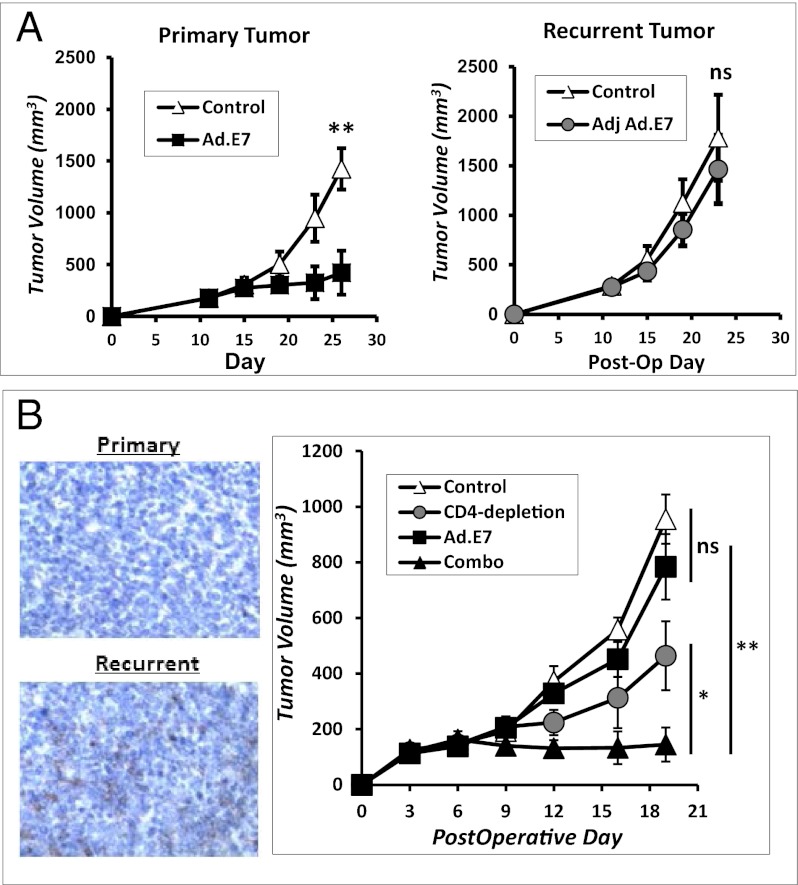
Each year, more than 700,000 people undergo cancer surgery in the United States. However, more than 40% of those patients develop recurrences and have a poor outcome. Traditionally, the medical community has assumed that recurrent tumors arise from selected tumor clones that are refractory to therapy. However, we found that tumor cells have few phenotypical differences after surgery. Thus, we propose an alternative explanation for the resistance of recurrent tumors. Surgery promotes inhibitory factors that allow lingering immunosuppressive cells to repopulate small pockets of residual disease quickly. Recurrent tumors and draining lymph nodes are infiltrated with M2 (CD11b(+)F4/80(hi)CD206(hi) and CD11b(+)F4/80(hi)CD124(hi)) macrophages and CD4(+)Foxp3(+) regulatory T cells. This complex network of immunosuppression in the surrounding tumor microenvironment explains the resistance of tumor recurrences to conventional cancer vaccines despite small tumor size, an intact antitumor immune response, and unaltered cancer cells. Therapeutic strategies coupling antitumor agents with inhibition of immunosuppressive cells potentially could impact the outcomes of more than 250,000 people each year.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60(5):277–300. - PubMed
-
- National Cancer Institute (2009) SEER Stat Database. (NCI, Bethesda)
-
- McCarter MD, Fong Y. Role for surgical cytoreduction in multimodality treatments for cancer. Ann Surg Oncol. 2001;8(1):38–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
