

Hyperoxic acute lung injury
- PMID: 23271823
- PMCID: PMC3915523
- DOI: 10.4187/respcare.01963
Hyperoxic acute lung injury
Abstract
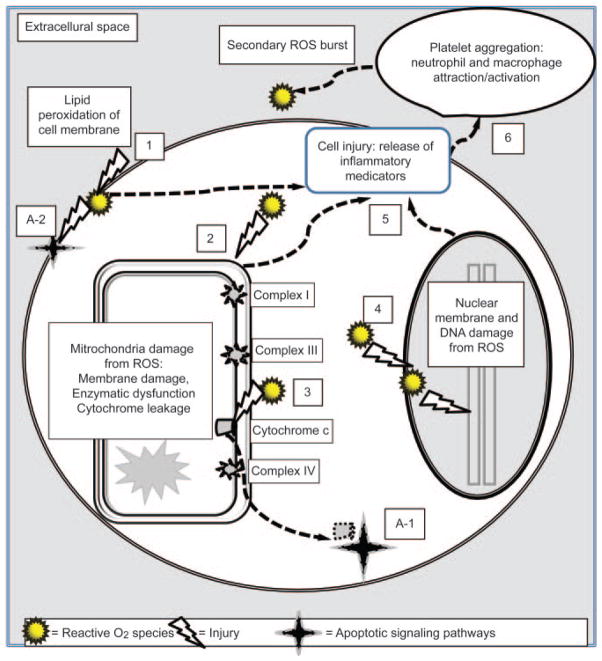
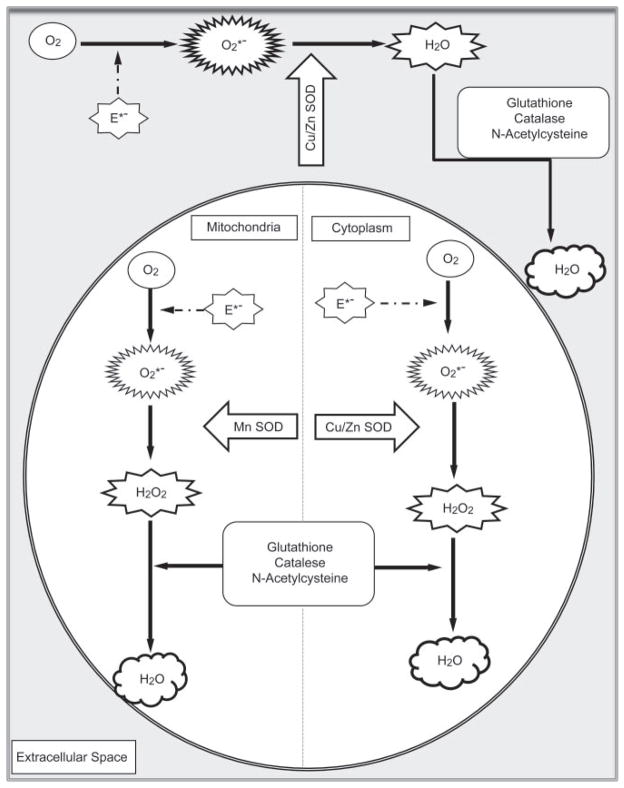
Prolonged breathing of very high F(IO(2)) (F(IO(2)) ≥ 0.9) uniformly causes severe hyperoxic acute lung injury (HALI) and, without a reduction of F(IO(2)), is usually fatal. The severity of HALI is directly proportional to P(O(2)) (particularly above 450 mm Hg, or an F(IO(2)) of 0.6) and exposure duration. Hyperoxia produces extraordinary amounts of reactive O(2) species that overwhelms natural anti-oxidant defenses and destroys cellular structures through several pathways. Genetic predisposition has been shown to play an important role in HALI among animals, and some genetics-based epidemiologic research suggests that this may be true for humans as well. Clinically, the risk of HALI likely occurs when F(IO(2)) exceeds 0.7, and may become problematic when F(IO(2)) exceeds 0.8 for an extended period of time. Both high-stretch mechanical ventilation and hyperoxia potentiate lung injury and may promote pulmonary infection. During the 1960s, confusion regarding the incidence and relevance of HALI largely reflected such issues as the primitive control of F(IO(2)), the absence of PEEP, and the fact that at the time both ALI and ventilator-induced lung injury were unknown. The advent of PEEP and precise control over F(IO(2)), as well as lung-protective ventilation, and other adjunctive therapies for severe hypoxemia, has greatly reduced the risk of HALI for the vast majority of patients requiring mechanical ventilation in the 21st century. However, a subset of patients with very severe ARDS requiring hyperoxic therapy is at substantial risk for developing HALI, therefore justifying the use of such adjunctive therapies.
Conflict of interest statement
The authors have disclosed no conflicts of interest.
Figures

References
-
- Bean JW. Effects of O2 at increased pressure. Physiol Rev. 1945;25(1):1–147.
-
- Ohlsson WTL. A study on O2 toxicity at atmospheric pressure with special reference to the pathogenesis of pulmonary damage and O2 O2 therapy. Acta Med Scand. 1947;190(Suppl):4–89.
-
- Clark JM, Lambertsen CJ. Pulmonary O2 toxicity: a review. Pharmacol Rev. 1971;23(2):37–133. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
