

Sequential anti-cytomegalovirus response monitoring may allow prediction of cytomegalovirus reactivation after allogeneic stem cell transplantation
- PMID: 23272059
- PMCID: PMC3521740
- DOI: 10.1371/journal.pone.0050248
Sequential anti-cytomegalovirus response monitoring may allow prediction of cytomegalovirus reactivation after allogeneic stem cell transplantation
Erratum in
- PLoS One. 2013;8(4). doi: 10.1371/annotation/43e9b84c-fbe3-4b39-88c8-1cde34b0afea
Abstract
Background: Reconstitution of cytomegalovirus-specific CD3(+)CD8(+) T cells (CMV-CTLs) after allogeneic hematopoietic stem cell transplantation (HSCT) is necessary to bring cytomegalovirus (CMV) reactivation under control. However, the parameters determining protective CMV-CTL reconstitution remain unclear to date.
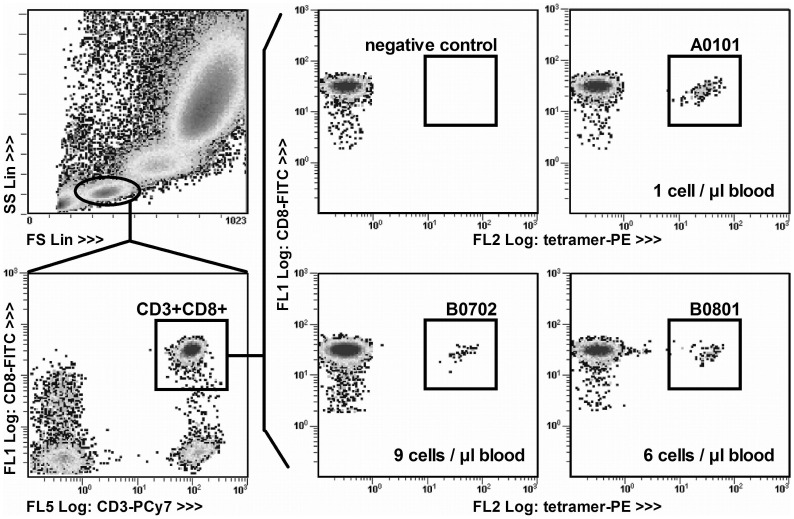
Design and methods: In a prospective tri-center study, CMV-CTL reconstitution was analyzed in the peripheral blood from 278 patients during the year following HSCT using 7 commercially available tetrameric HLA-CMV epitope complexes. All patients included could be monitored with at least CMV-specific tetramer.
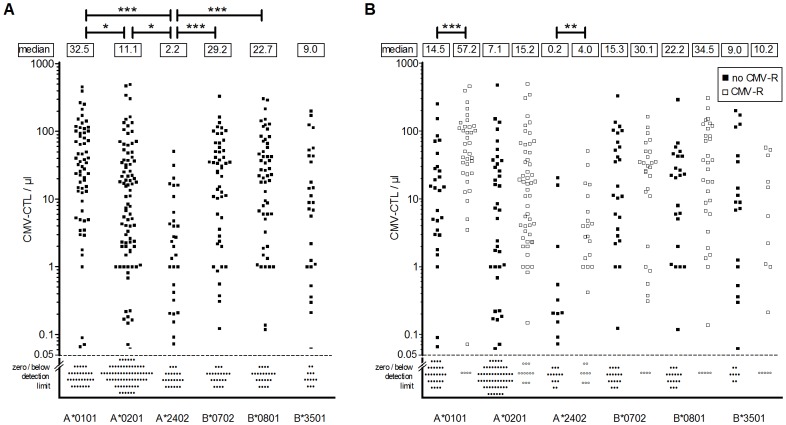
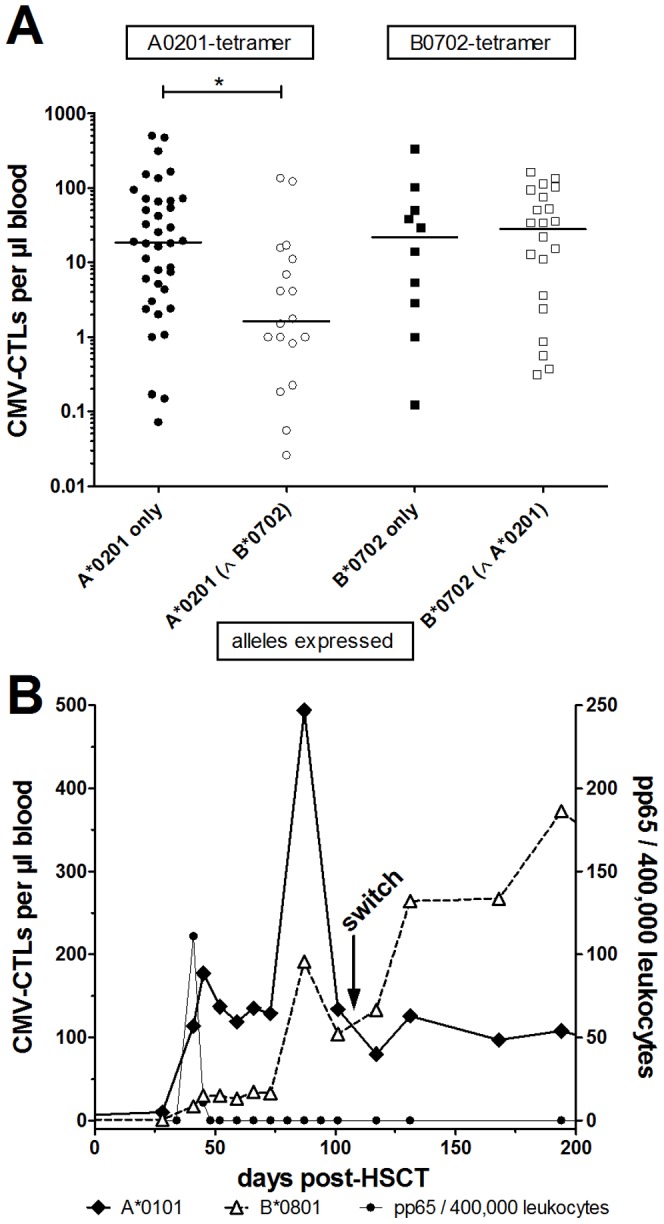
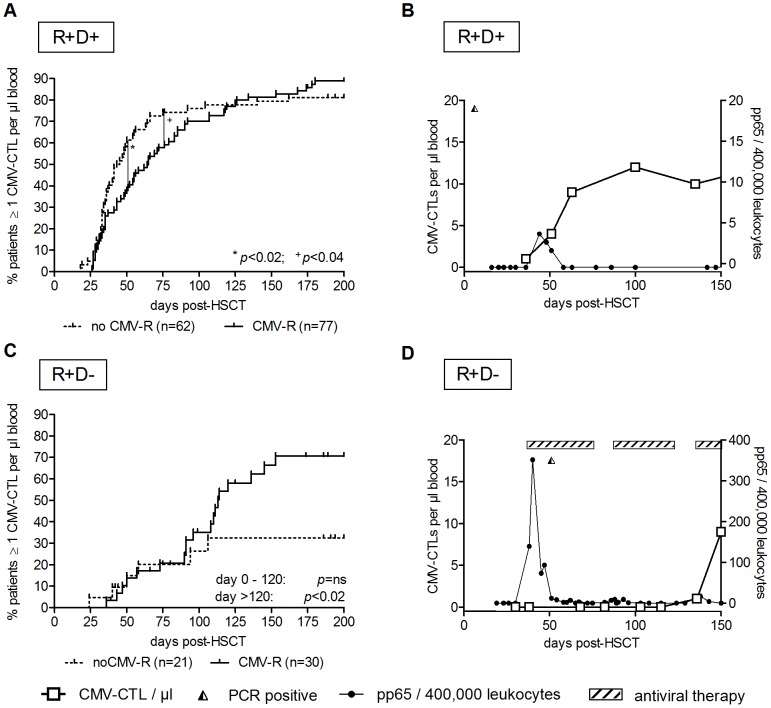
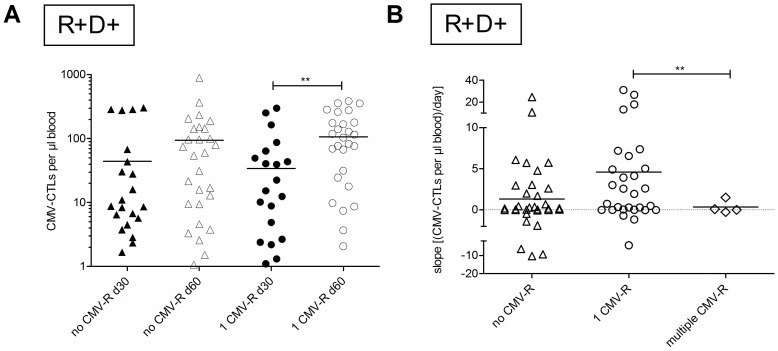
Results: CMV-CTL reconstitution was detected in 198 patients (71%) after allogeneic HSCT. Most importantly, reconstitution with 1 CMV-CTL per µl blood between day +50 and day +75 post-HSCT discriminated between patients with and without CMV reactivation in the R+/D+ patient group, independent of the CMV-epitope recognized. In addition, CMV-CTLs expanded more daramtaically in patients experiencing only one CMV-reactivation than those without or those with multiple CMV reactivations. Monitoring using at least 2 tetramers was possible in 63% (n = 176) of the patients. The combinations of particular HLA molecules influenced the numbers of CMV-CTLs detected. The highest CMV-CTL count obtained for an individual tetramer also changed over time in 11% of these patients (n = 19) resulting in higher levels of HLA-B*0801 (IE-1) recognizing CMV-CTLs in 14 patients.
Conclusions: Our results indicate that 1 CMV-CTL per µl blood between day +50 to +75 marks the beginning of an immune response against CMV in the R+/D+ group. Detection of CMV-CTL expansion thereafter indicates successful resolution of the CMV reactivation. Thus, sequential monitoring of CMV-CTL reconstitution can be used to predict patients at risk for recurrent CMV reactivation.
Conflict of interest statement
Figures
Similar articles
-
Tetramer monitoring to assess risk factors for recurrent cytomegalovirus reactivation and reconstitution of antiviral immunity post allogeneic hematopoietic stem cell transplantation.Transpl Infect Dis. 2011 Jun;13(3):222-36. doi: 10.1111/j.1399-3062.2011.00626.x. Epub 2011 May 18. Transpl Infect Dis. 2011. PMID: 21585633
-
Protective immunity transferred by infusion of cytomegalovirus-specific CD8(+) T cells within donor grafts: its associations with cytomegalovirus reactivation following unmanipulated allogeneic hematopoietic stem cell transplantation.Biol Blood Marrow Transplant. 2010 Jul;16(7):994-1004. doi: 10.1016/j.bbmt.2010.02.007. Epub 2010 Feb 16. Biol Blood Marrow Transplant. 2010. PMID: 20167279
-
Reconstitution of cytomegalovirus specific T cells after pediatric allogeneic stem cell transplantation: results from a pilot study using a multi-allele CMV tetramer group.Klin Padiatr. 2008 Nov-Dec;220(6):348-52. doi: 10.1055/s-0028-1086029. Epub 2008 Oct 23. Klin Padiatr. 2008. PMID: 18949669
-
Prevention of cytomegalovirus disease in recipients of allogeneic stem cell transplants.Clin Microbiol Rev. 2003 Oct;16(4):647-57. doi: 10.1128/CMR.16.4.647-657.2003. Clin Microbiol Rev. 2003. PMID: 14557291 Free PMC article. Review.
-
Control of Cytomegalovirus Viremia after Allogeneic Stem Cell Transplantation: A Review on CMV-Specific T Cell Reconstitution.Biol Blood Marrow Transplant. 2018 Sep;24(9):1776-1782. doi: 10.1016/j.bbmt.2018.03.028. Epub 2018 Apr 4. Biol Blood Marrow Transplant. 2018. PMID: 29626514 Review.
Cited by
-
Comparison of cytomegalovirus (CMV) enzyme-linked immunosorbent spot and CMV quantiferon gamma interferon-releasing assays in assessing risk of CMV infection in kidney transplant recipients.J Clin Microbiol. 2013 Aug;51(8):2501-7. doi: 10.1128/JCM.00563-13. Epub 2013 May 15. J Clin Microbiol. 2013. PMID: 23678073 Free PMC article.
-
The immune response to cytomegalovirus in allogeneic hematopoietic stem cell transplant recipients.Cell Mol Life Sci. 2015 Nov;72(21):4049-62. doi: 10.1007/s00018-015-1986-z. Epub 2015 Jul 15. Cell Mol Life Sci. 2015. PMID: 26174234 Free PMC article. Review.
-
Standardized monitoring of cytomegalovirus-specific immunity can improve risk stratification of recurrent cytomegalovirus reactivation after hematopoietic stem cell transplantation.Haematologica. 2021 Feb 1;106(2):363-374. doi: 10.3324/haematol.2019.229252. Haematologica. 2021. PMID: 31879324 Free PMC article.
-
Immune Reconstitution after Allogeneic Hematopoietic Stem Cell Transplantation.Front Immunol. 2016 Nov 17;7:507. doi: 10.3389/fimmu.2016.00507. eCollection 2016. Front Immunol. 2016. PMID: 27909435 Free PMC article. Review.
-
Adaptive NK cells undergo a dynamic modulation in response to human cytomegalovirus and recruit T cells in in vitro migration assays.Bone Marrow Transplant. 2022 May;57(5):712-720. doi: 10.1038/s41409-022-01603-y. Epub 2022 Feb 17. Bone Marrow Transplant. 2022. PMID: 35177828 Free PMC article.
References
-
- Mori T, Kato J (2010) Cytomegalovirus infection/disease after hematopoietic stem cell transplantation. Int J Hematol 91: 588–595. - PubMed
-
- Boeckh M, Nichols WG, Papanicolaou G, Rubin R, Wingard JR, et al. (2003) Cytomegalovirus in hematopoietic stem cell transplant recipients: Current status, known challenges, and future strategies. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation 9: 543–558. - PubMed
-
- Hebart H, Einsele H (2004) Clinical aspects of CMV infection after stem cell transplantation. Hum Immunol 65: 432–436. - PubMed
-
- Torres HA, Aguilera E, Safdar A, Rohatgi N, Raad II, et al. (2008) Fatal cytomegalovirus pneumonia in patients with haematological malignancies: an autopsy-based case-control study. Clin Microbiol Infect 14: 1160–1166. - PubMed
-
- Ljungman P, Griffiths P, Paya C (2002) Definitions of cytomegalovirus infection and disease in transplant recipients. Clin Infect Dis 34: 1094–1097. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
