

Capacity-building and clinical competence in infectious disease in Uganda: a mixed-design study with pre/post and cluster-randomized trial components
- PMID: 23272097
- PMCID: PMC3522731
- DOI: 10.1371/journal.pone.0051319
Capacity-building and clinical competence in infectious disease in Uganda: a mixed-design study with pre/post and cluster-randomized trial components
Abstract
Trial design: Best practices for training mid-level practitioners (MLPs) to improve global health-services are not well-characterized. Two hypotheses were: 1) Integrated Management of Infectious Disease (IMID) training would improve clinical competence as tested with a single arm, pre-post design, and 2) on-site support (OSS) would yield additional improvements as tested with a cluster-randomized trial.
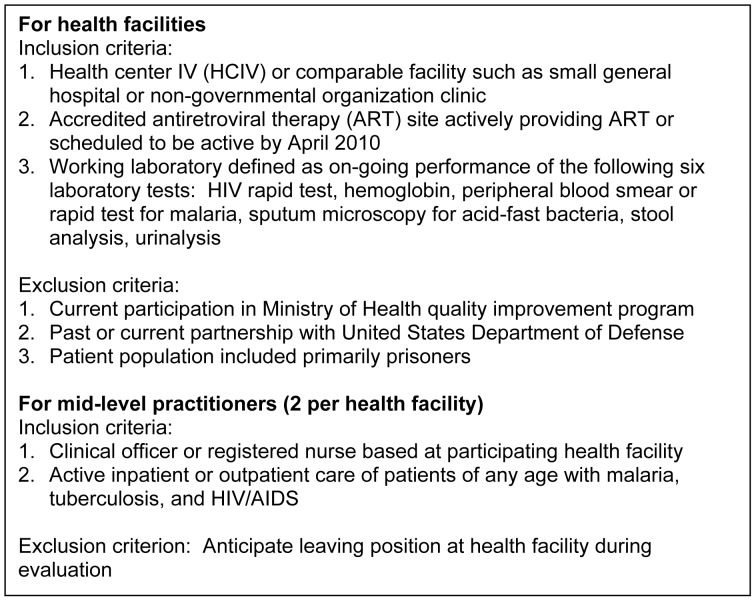
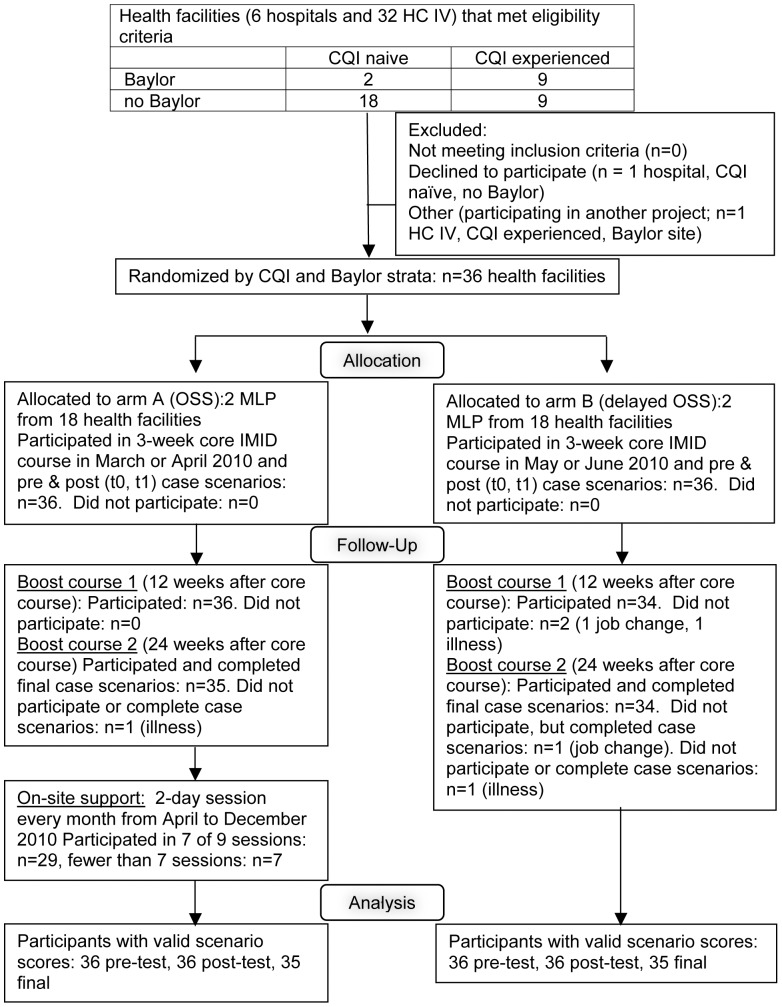
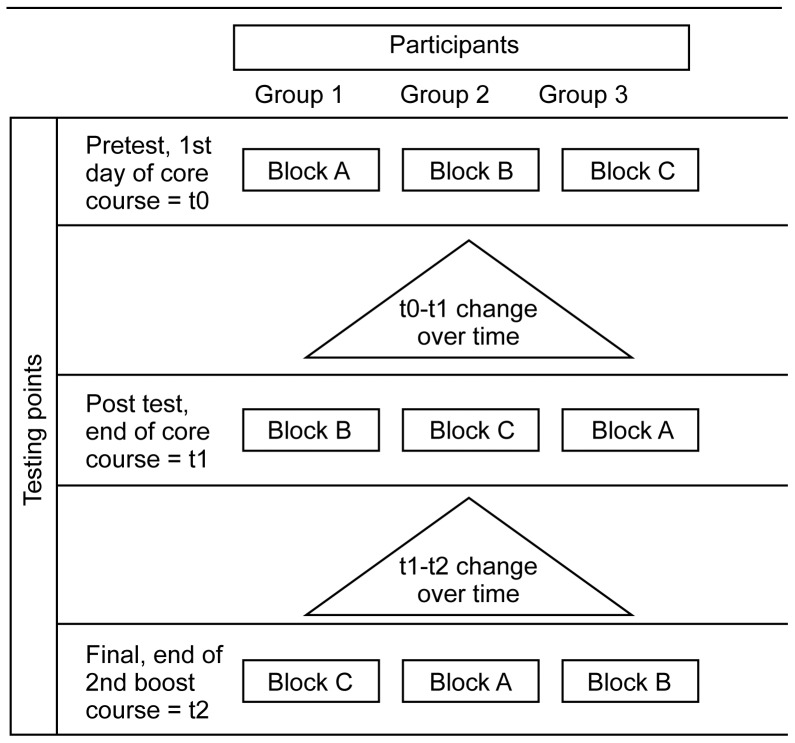
Methods: Thirty-six Ugandan health facilities (randomized 1∶1 to parallel OSS and control arms) enrolled two MLPs each. All MLPs participated in IMID (3-week core course, two 1-week boost sessions, distance learning). After the 3-week course, OSS-arm trainees participated in monthly OSS. Twelve written case scenarios tested clinical competencies in HIV/AIDS, tuberculosis, malaria, and other infectious diseases. Each participant completed different randomly-assigned blocks of four scenarios before IMID (t0), after 3-week course (t1), and after second boost course (t2, 24 weeks after t1). Scoring guides were harmonized with IMID content and Ugandan national policy. Score analyses used a linear mixed-effects model. The primary outcome measure was longitudinal change in scenario scores.
Results: Scores were available for 856 scenarios. Mean correct scores at t0, t1, and t2 were 39.3%, 49.1%, and 49.6%, respectively. Mean score increases (95% CI, p-value) for t0-t1 (pre-post period) and t1-t2 (parallel-arm period) were 12.1 ((9.6, 14.6), p<0.001) and -0.6 ((-3.1, +1.9), p = 0.647) percent for OSS arm and 7.5 ((5.0, 10.0), p<0.001) and 1.6 ((-1.0, +4.1), p = 0.225) for control arm. The estimated mean difference in t1 to t2 score change, comparing arm A (participated in OSS) vs. arm B was -2.2 ((-5.8, +1.4), p = 0.237). From t0-t2, mean scores increased for all 12 scenarios.
Conclusions: Clinical competence increased significantly after a 3-week core course; improvement persisted for 24 weeks. No additional impact of OSS was observed. Data on clinical practice, facility-level performance and health outcomes will complete assessment of overall impact of IMID and OSS.
Trial registration: ClinicalTrials.gov NCT01190540.
Conflict of interest statement
Figures
References
-
- Committee on the U.S. Commitment to Global Health; Institute of Medicine (2009) The U.S. commitment to global health: Recommendations for the public and private sectors. Washington, DC: Institute of Medicine.
-
- Hirschhorn LR, Oguda L, Fullem A, Dreesch N, Wilson P (2006) Estimating health workforce needs for antiretroviral therapy in resource-limited settings. Hum Resour Health 4: 1 doi:10.1186/1478-4491-4-1. - DOI - PMC - PubMed
-
- Laserson KF, Osorio L, Sheppard JD, Hernández H, Benítez AM, et al. (2000) Clinical and programmatic mismanagement rather than community outbreak as the cause of chronic, drug-resistant tuberculosis in Buenaventura, Colombia, 1998. Int J Tuberc Lung Dis 4: 673–683. - PubMed
-
- Nankabirwa J, Zurovac D, Njogu JN, Rwakimari JB, Counihan H, et al. (2009) Malaria misdiagnosis in Uganda – implications for policy change. Malar J 8: 66 doi:10.1186/1475-2875-8-66. - DOI - PMC - PubMed
-
- Brentlinger PE, Vallejo Torres J, Martínez PM, Ghee A, Lujan J, et al. (2010) Clinical staging of HIV-related illness in Mozambique: Performance of non-physician clinicians based on direct observation of clinical care, and implications for health-worker training. J Acquir Immune Defic Synd 55: 351–5. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
