

Degree of skin denervation and its correlation to objective thermal sensory test in leprosy patients
- PMID: 23272267
- PMCID: PMC3521713
- DOI: 10.1371/journal.pntd.0001975
Degree of skin denervation and its correlation to objective thermal sensory test in leprosy patients
Abstract
Background: Leprosy is an infectious disease affecting skin and peripheral nerves resulting in increased morbidity and physical deformities. Early diagnosis provides opportune treatment and reduces its complications, relying fundamentally on the demonstration of impaired sensation in suggestive cutaneous lesions. The loss of tactile sensitivity in the lesions is preceded by the loss of thermal sensitivity, stressing the importance of the thermal test in the suspicious lesions approach. The gold-standard method for the assessment of thermal sensitivity is the quantitative sensory test (QST). Morphological study may be an alternative approach to access the thin nerve fibers responsible for thermal sensitivity transduction. The few studies reported in leprosy patients pointed out a rarefaction of thin dermo-epidermal fibers in lesions, but used semi-quantitative evaluation methods.
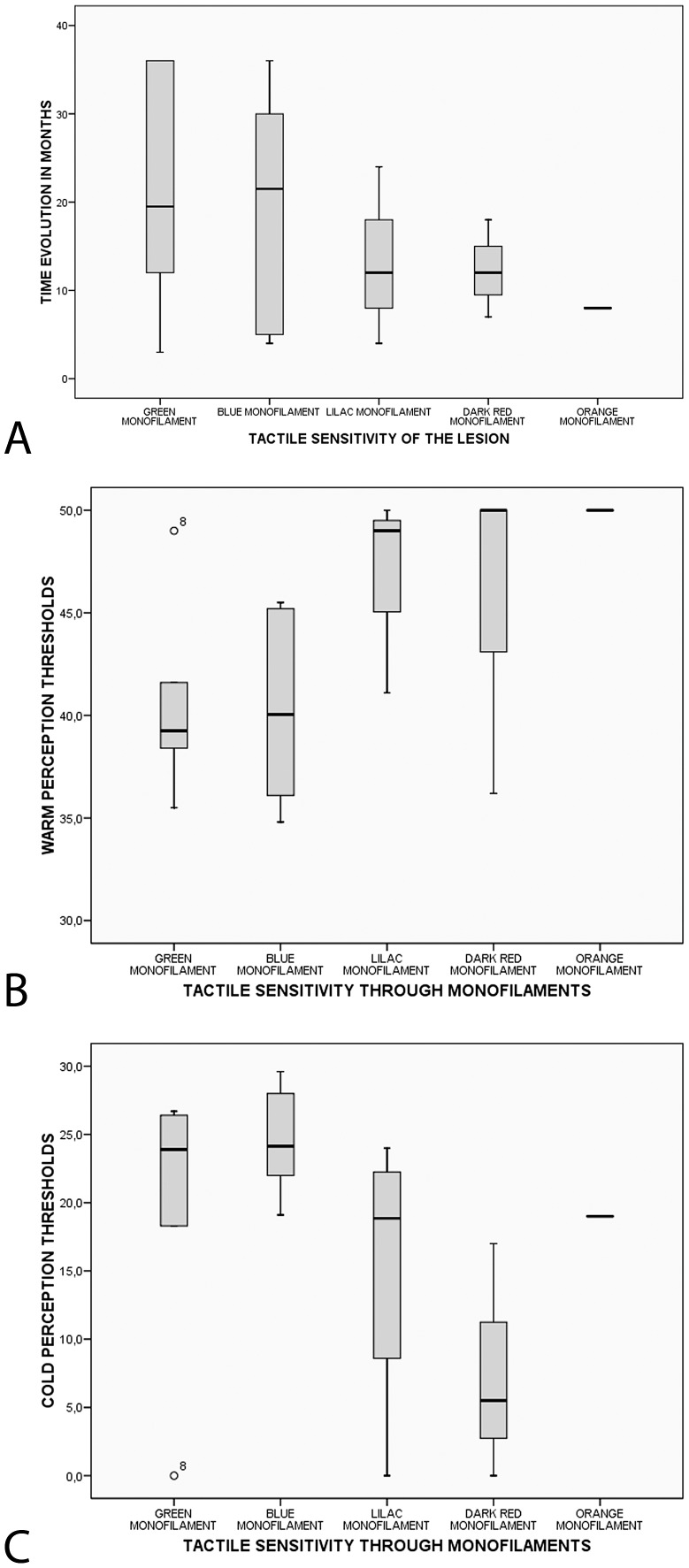
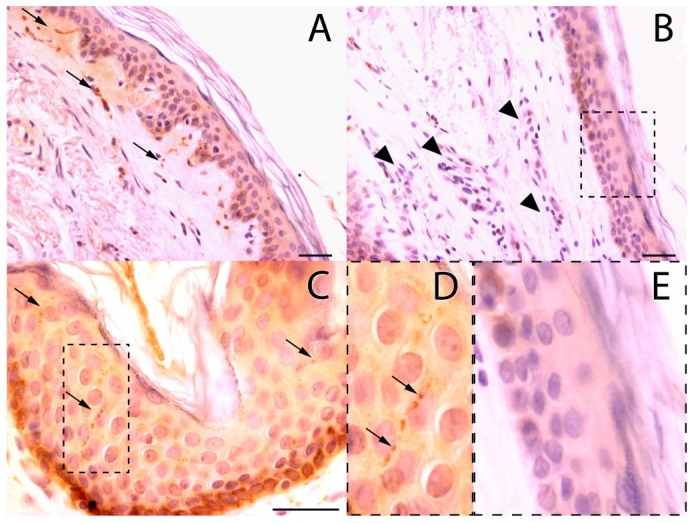
Methodology/principal findings: This work aimed to study the correlation between the degree of thermal sensitivity impairment measured by QST and the degree of denervation in leprosy skin lesions, evaluated by immunohistochemistry anti-PGP 9.5 and morphometry. Twenty-two patients were included. There were significant differences in skin thermal thresholds among lesions and contralateral skin (cold, warm, cold induced pain and heat induced pain). The mean reduction in the density of intraepidermal and subepidermal fibers in lesions was 79.5% (SD = 19.6) and 80.8% (SD = 24.9), respectively.
Conclusions/significance: We observed a good correlation between intraepidermal and subepidermal fibers deficit, but no correlation between these variables and those accounting for the degree of impairment in thermal thresholds, since the thin fibers rarefaction was homogeneously intense in all patients, regardless of the degree of sensory deficit. We believe that the homogeneously intense denervation in leprosy lesions should be objective of further investigations focused on its diagnostic applicability, particularly in selected cases with only discrete sensory impairment, patients unable to perform the sensory test and especially those with nonspecific histopathological finds.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Detection of sensory deficits in fine nerve fibres in leprosy diagnosis.Trop Med Int Health. 2025 Mar;30(3):170-180. doi: 10.1111/tmi.14079. Epub 2025 Jan 9. Trop Med Int Health. 2025. PMID: 39788712
-
Correlation of quantitative tests of nerve and target organ dysfunction with skin immunohistology in leprosy.Brain. 1998 Dec;121 ( Pt 12):2239-47. doi: 10.1093/brain/121.12.2239. Brain. 1998. PMID: 9874477
-
Cutaneous lesions sensory impairment recovery and nerve regeneration in leprosy patients.Mem Inst Oswaldo Cruz. 2012 Dec;107 Suppl 1:68-73. doi: 10.1590/s0074-02762012000900012. Mem Inst Oswaldo Cruz. 2012. PMID: 23283456
-
Comparative study of the cutaneous sensation of leprosy-suspected lesions using Semmes-Weinstein monofilaments and quantitative thermal testing.Lepr Rev. 2007 Jun;78(2):102-9. Lepr Rev. 2007. PMID: 17824480
-
Impaired warm and cold perception thresholds in leprosy skin lesions.Lepr Rev. 2007 Jun;78(2):110-21. Lepr Rev. 2007. PMID: 17824481
Cited by
-
C-Fiber Assays in the Cornea vs. Skin.Brain Sci. 2019 Nov 12;9(11):320. doi: 10.3390/brainsci9110320. Brain Sci. 2019. PMID: 31718074 Free PMC article. Review.
-
Treatment and Evaluation Advances in Leprosy Neuropathy.Neurotherapeutics. 2021 Oct;18(4):2337-2350. doi: 10.1007/s13311-021-01153-z. Epub 2021 Nov 19. Neurotherapeutics. 2021. PMID: 34799845 Free PMC article. Review.
-
Neural leprosy investigation using electroneuromyography and the ML Flow rapid test: a case report.Rev Soc Bras Med Trop. 2024 Feb 12;57:e008022024. doi: 10.1590/0037-8682-0586-2023. eCollection 2024. Rev Soc Bras Med Trop. 2024. PMID: 38359312 Free PMC article.
-
Relationship between Plantar Pressure and Sensory Disturbance in Patients with Hansen's Disease-Preliminary Research and Review of the Literature.Sensors (Basel). 2020 Dec 6;20(23):6976. doi: 10.3390/s20236976. Sensors (Basel). 2020. PMID: 33291332 Free PMC article. Review.
References
-
- Araújo M (2003) Leprosy in Brazil. Rev Soc Bras Med Trop 36 3: 373–382. - PubMed
-
- Goulart IMB, Goulart LR (2008) Leprosy: diagnostic and control challenges for a worldwide disease. Arch Dermatol Res 300 6: 269–290. - PubMed
-
- Moschella SL (2004) An update on the diagnosis and treatment of leprosy. J Am Acad Dermatol 51 3: 417–426. - PubMed
-
- Walker SL, Lockwood DNJ (2007) Leprosy. Clin Dermatol 25 2: 165–172. - PubMed
-
- Agrawal A, Pandit L, Dalal M, Shetty JP (2005) Neurological manifestations of Hansen's disease and their management. Clin Neurol Neurosurg 107 6: 445–454. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
