

Outcome at two years of age in a Swiss national cohort of extremely preterm infants born between 2000 and 2008
- PMID: 23272671
- PMCID: PMC3546845
- DOI: 10.1186/1471-2431-12-198
Outcome at two years of age in a Swiss national cohort of extremely preterm infants born between 2000 and 2008
Abstract
Background: While survival rates of extremely preterm infants have improved over the last decades, the incidence of neurodevelopmental disability (ND) in survivors remains high. Representative current data on the severity of disability and of risk factors associated with poor outcome in this growing population are necessary for clinical guidance and parent counselling.
Methods: Prospective longitudinal multicentre cohort study of preterm infants born in Switzerland between 24(0/7) and 27(6/7) weeks gestational age during 2000-2008. Mortality, adverse outcome (death or severe ND) at two years, and predictors for poor outcome were analysed using multilevel multivariate logistic regression. Neurodevelopment was assessed using Bayley Scales of Infant Development II. Cerebral palsy was graded after the Gross Motor Function Classification System.
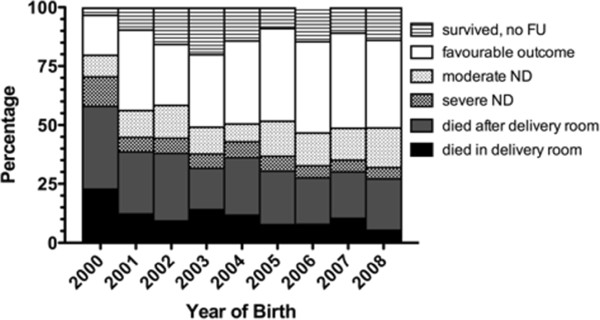
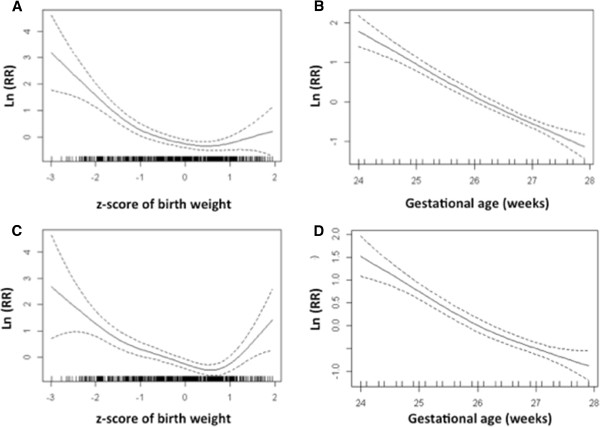
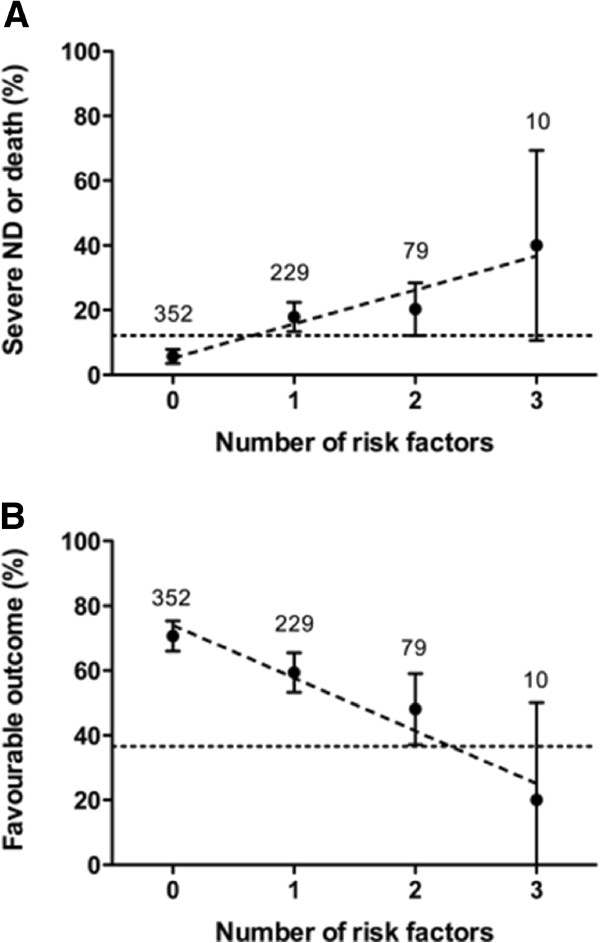
Results: Of 1266 live born infants, 422 (33%) died. Follow-up information was available for 684 (81%) survivors: 440 (64%) showed favourable outcome, 166 (24%) moderate ND, and 78 (11%) severe ND. At birth, lower gestational age, intrauterine growth restriction and absence of antenatal corticosteroids were associated with mortality and adverse outcome (p < 0.001). At 36(0/7) weeks postmenstrual age, bronchopulmonary dysplasia, major brain injury and retinopathy of prematurity were the main predictors for adverse outcome (p < 0.05). Survival without moderate or severe ND increased from 27% to 39% during the observation period (p = 0.02).
Conclusions: In this recent Swiss national cohort study of extremely preterm infants, neonatal mortality was determined by gestational age, birth weight, and antenatal corticosteroids while neurodevelopmental outcome was determined by the major neonatal morbidities. We observed an increase of survival without moderate or severe disability.
Figures
References
-
- Fanaroff AA, Stoll BJ, Wright LL, Carlo WA, Ehrenkranz RA, Stark AR. et al.Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol. 2007;196(2):e147–e141. 148. - PubMed
