

Diffuse myocardial fibrosis evaluation using cardiac magnetic resonance T1 mapping: sample size considerations for clinical trials
- PMID: 23272704
- PMCID: PMC3552738
- DOI: 10.1186/1532-429X-14-90
Diffuse myocardial fibrosis evaluation using cardiac magnetic resonance T1 mapping: sample size considerations for clinical trials
Abstract
Background: Cardiac magnetic resonance (CMR) T1 mapping has been used to characterize myocardial diffuse fibrosis. The aim of this study is to determine the reproducibility and sample size of CMR fibrosis measurements that would be applicable in clinical trials.
Methods: A modified Look-Locker with inversion recovery (MOLLI) sequence was used to determine myocardial T1 values pre-, and 12 and 25min post-administration of a gadolinium-based contrast agent at 3 Tesla. For 24 healthy subjects (8 men; 29 ± 6 years), two separate scans were obtained a) with a bolus of 0.15mmol/kg of gadopentate dimeglumine and b) 0.1mmol/kg of gadobenate dimeglumine, respectively, with averaged of 51 ± 34 days between two scans. Separately, 25 heart failure subjects (12 men; 63 ± 14 years), were evaluated after a bolus of 0.15mmol/kg of gadopentate dimeglumine. Myocardial partition coefficient (λ) was calculated according to (ΔR1myocardium/ΔR1blood), and ECV was derived from λ by adjusting (1-hematocrit).
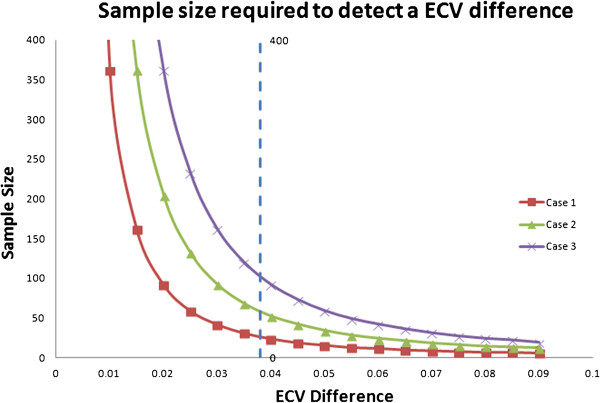
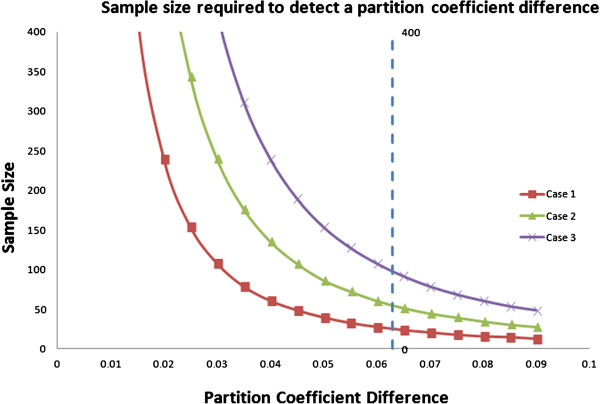
Results: Mean ECV and λ were both significantly higher in HF subjects than healthy (ECV: 0.287 ± 0.034 vs. 0.267 ± 0.028, p=0.002; λ: 0.481 ± 0.052 vs. 442 ± 0.037, p < 0.001, respectively). The inter-study ECV and λ variation were about 2.8 times greater than the intra-study ECV and λ variation in healthy subjects (ECV:0.017 vs. 0.006, λ:0.025 vs. 0.009, respectively). The estimated sample size to detect ECV change of 0.038 or λ change of 0.063 (corresponding to ~3% increase of histological myocardial fibrosis) with a power of 80% and an alpha error of 0.05 for heart failure subjects using a two group design was 27 in each group, respectively.
Conclusion: ECV and λ quantification have a low variability across scans, and could be a viable tool for evaluating clinical trial outcome.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
