

Ultrasound assessment of lower limb muscle mass in response to resistance training in COPD
- PMID: 23273255
- PMCID: PMC3560243
- DOI: 10.1186/1465-9921-13-119
Ultrasound assessment of lower limb muscle mass in response to resistance training in COPD
Abstract
Background: Quantifying the improvements in lower limb or quadriceps muscle mass following resistance training (RT), is an important outcome measure in COPD. Ultrasound is a portable, radiation free imaging technique that can measure the size of superficial muscles belonging to the quadriceps group such as the rectus femoris, but has not been previously used in COPD patients following RT. We compared the responsiveness of ultrasound derived measures of quadriceps mass against dual energy x-ray absorptiometry (DEXA), in patients with COPD and healthy controls following a programme of high intensity knee extensor RT.
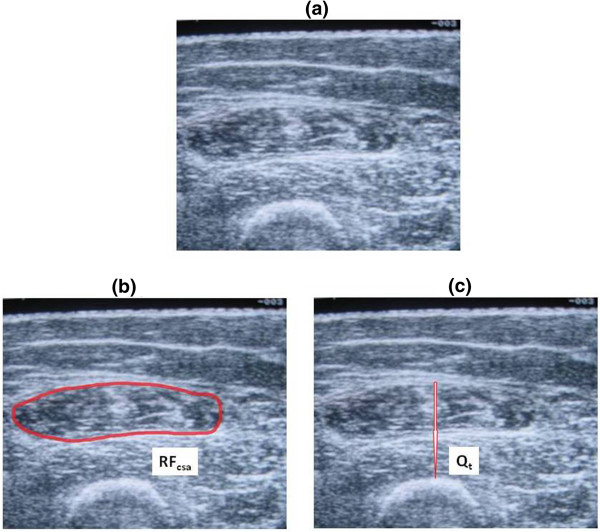
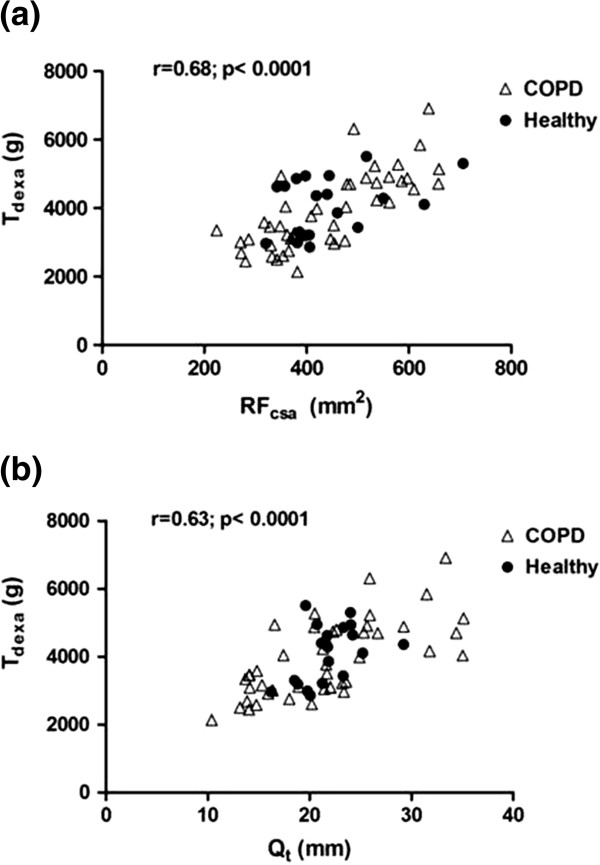
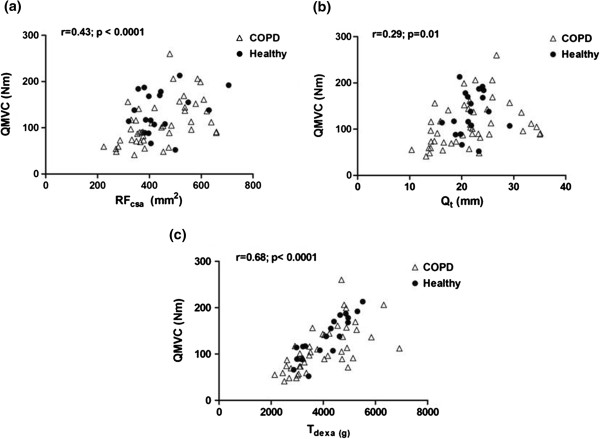
Methods: Portable ultrasound was used to assess the size of the dominant quadriceps in 45 COPD patients and 19 healthy controls-before, during, and after 8 weeks of bilateral high intensity isokinetic knee extensor RT. Scanning was performed at the mid-thigh region, and 2 indices of quadriceps mass were measured-rectus femoris cross-sectional area (RFcsa) and quadriceps muscle thickness (Qt). Thigh lean mass (Tdexa) was determined by DEXA.
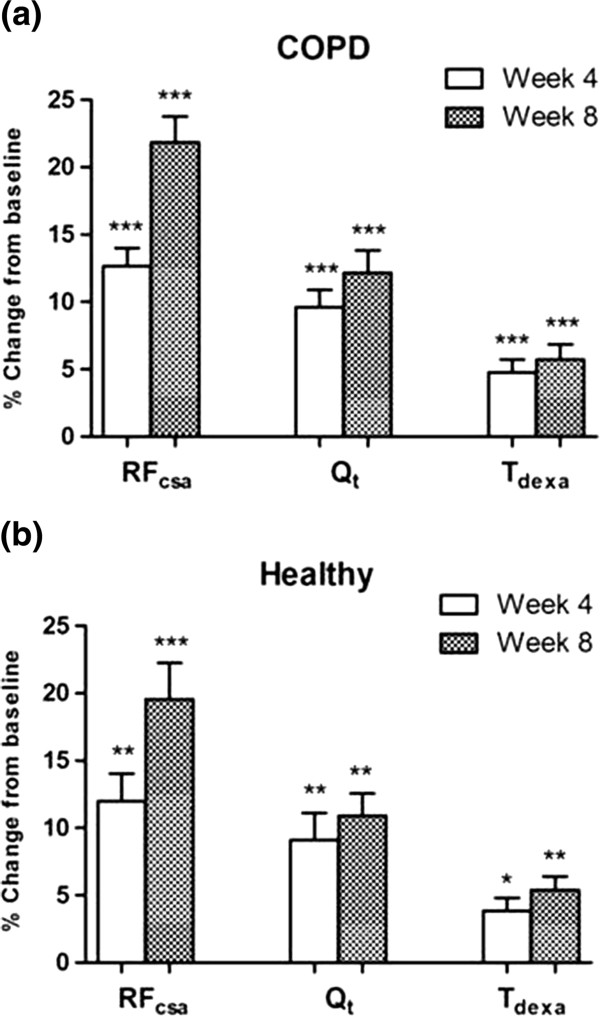
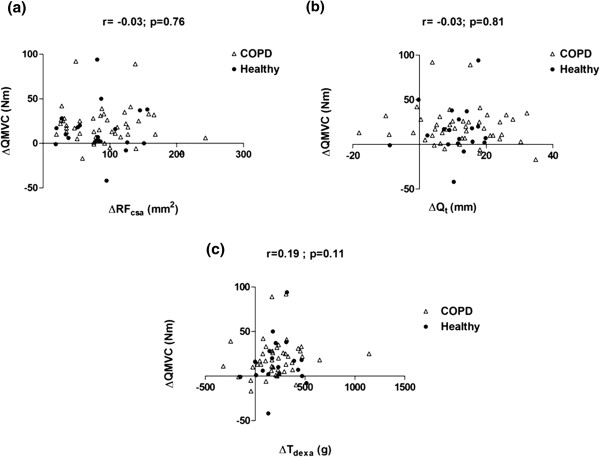
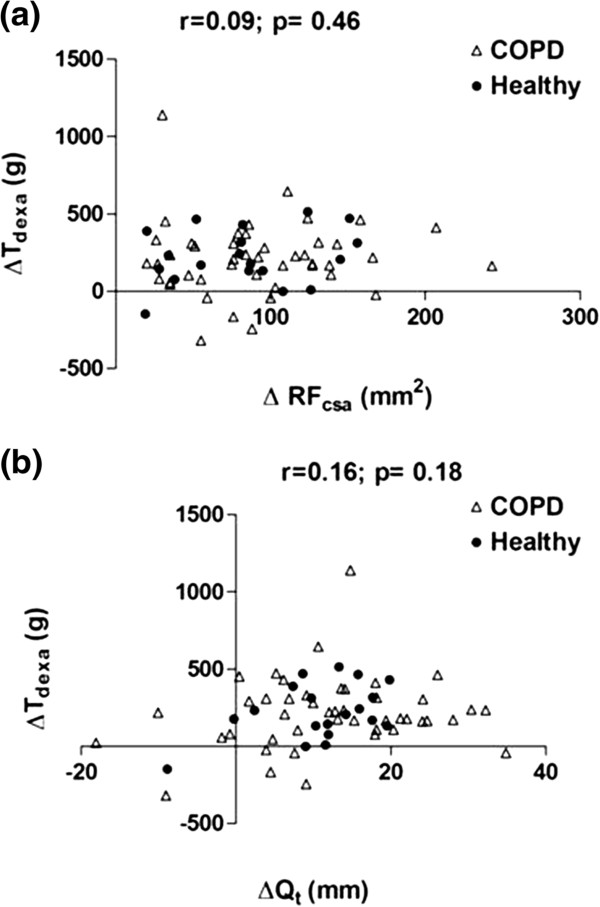
Results: Training resulted in a significant increase in Tdexa, RFcsa and Qt in COPD patients [5.7%, 21.8%, 12.1% respectively] and healthy controls [5.4%, 19.5%, 10.9 respectively]. The effect size for the changes in RFcsa (COPD= 0.77; Healthy=0.83) and Qt (COPD=0.36; Healthy=0.78) were greater than the changes in Tdexa (COPD=0.19; Healthy=0.26) following RT.
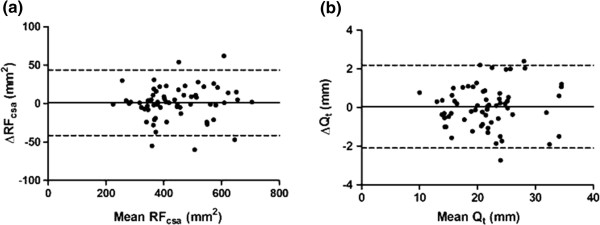
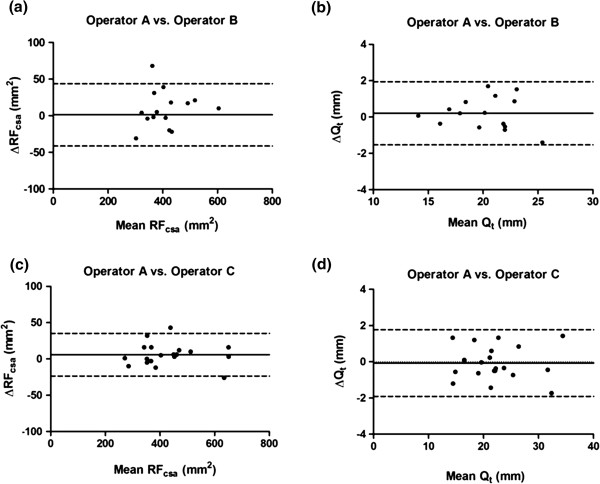
Conclusions: Serial ultrasound measurements of the quadriceps can detect changes in muscle mass in response to RT in COPD. The technique has good reproducibility, and may be more sensitive to changes in muscle mass when compared to DEXA.
Trial registration: http://www.controlled-trials.com (Identifier: ISRCTN22764439).
Figures
References
-
- Gosselink R, Troosters T, Decramer M. Peripheral muscle weakness contributes to exercise limitation in COPD. Am J Respir Crit Care Med. 1996;153:976–980. - PubMed
-
- Marquis K, Debigare R, Lacasse Y, Leblanc P, Jobin J, Carrier G. et al. Midthigh muscle cross-sectional area is a better predictor of mortality than body mass index in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166:809–813. doi: 10.1164/rccm.2107031. - DOI - PubMed
-
- Bernard S, Whittom F, Leblanc P, Jobin J, Belleau R, Berube C. et al. Aerobic and strength training in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;159:896–901. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
