

Influence of bacterial interactions on pneumococcal colonization of the nasopharynx
- PMID: 23273566
- PMCID: PMC3729046
- DOI: 10.1016/j.tim.2012.11.005
Influence of bacterial interactions on pneumococcal colonization of the nasopharynx
Abstract
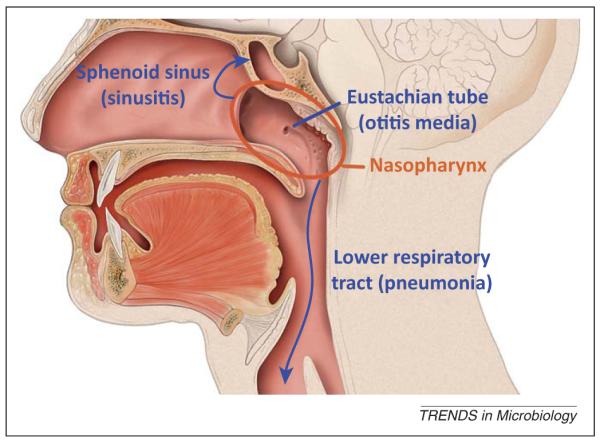
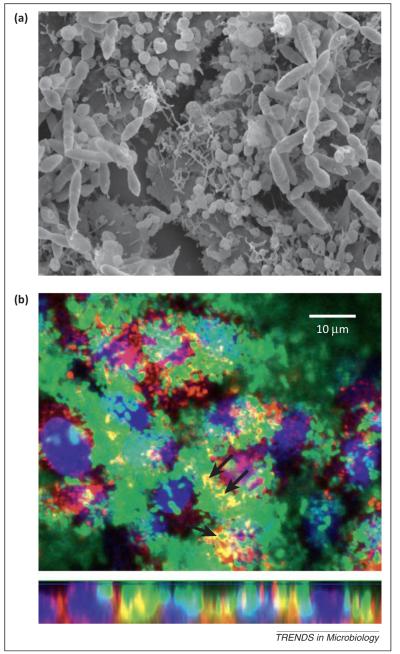
Streptococcus pneumoniae (the pneumococcus) is a common commensal inhabitant of the nasopharynx and a frequent etiologic agent in serious diseases such as pneumonia, otitis media, bacteremia, and meningitis. Multiple pneumococcal strains can colonize the nasopharynx, which is also home to many other bacterial species. Intraspecies and interspecies interactions influence pneumococcal carriage in important ways. Co-colonization by two or more pneumococcal strains has implications for vaccine serotype replacement, carriage detection, and pneumonia diagnostics. Interactions between the pneumococcus and other bacterial species alter carriage prevalence, modulate virulence, and affect biofilm formation. By examining these interactions, this review highlights how the bacterial ecosystem of the nasopharynx changes the nature and course of pneumococcal carriage.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
References
-
- van der Poll T, Opal SM. Pathogenesis, treatment, and prevention of pneumococcal pneumonia. Lancet. 2009;374:1543–1556. - PubMed
-
- O’Brien KL, et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet. 2009;374:893–902. - PubMed
-
- Huang SS, et al. Healthcare utilization and cost of pneumococcal disease in the United States. Vaccine. 2011;29:3398–3412. - PubMed
-
- Bogaert D, et al. Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect. Dis. 2004;4:144–154. - PubMed
-
- Simell B, et al. The fundamental link between pneumococcal carriage and disease. Expert Rev. Vaccines. 2012;11:841–855. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
