

Congenital hyperinsulinism caused by hexokinase I expression or glucokinase-activating mutation in a subset of β-cells
- PMID: 23274908
- PMCID: PMC3636634
- DOI: 10.2337/db12-1414
Congenital hyperinsulinism caused by hexokinase I expression or glucokinase-activating mutation in a subset of β-cells
Abstract
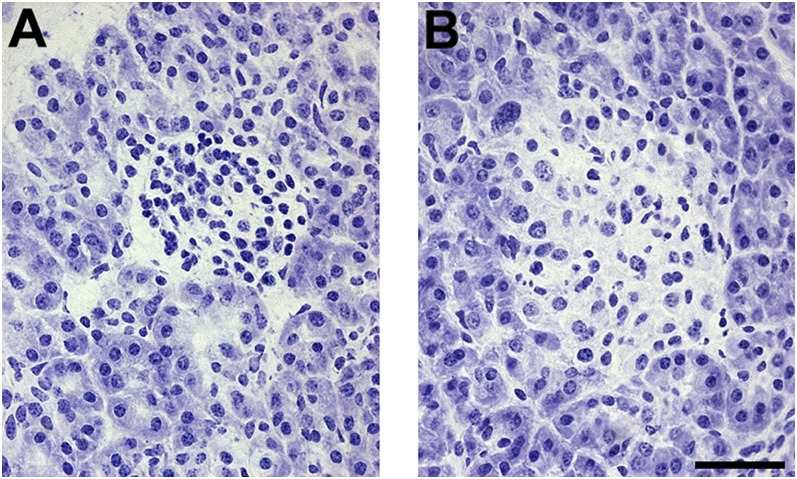
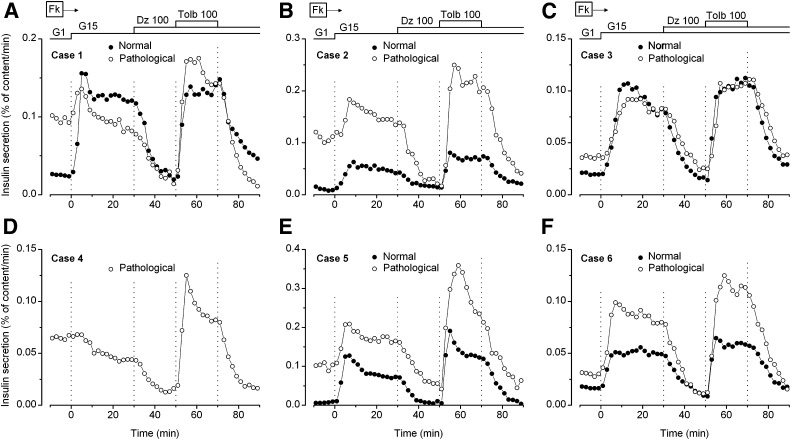
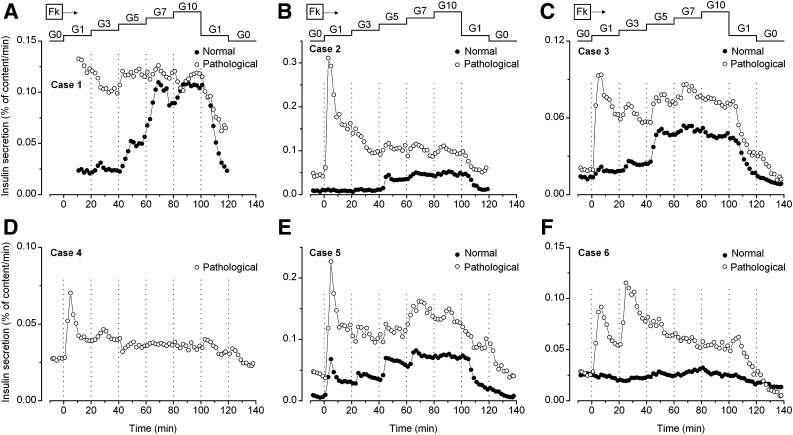
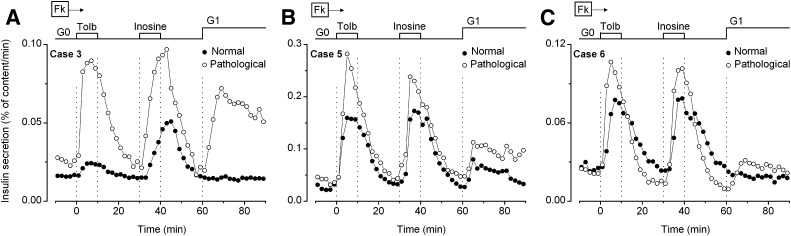
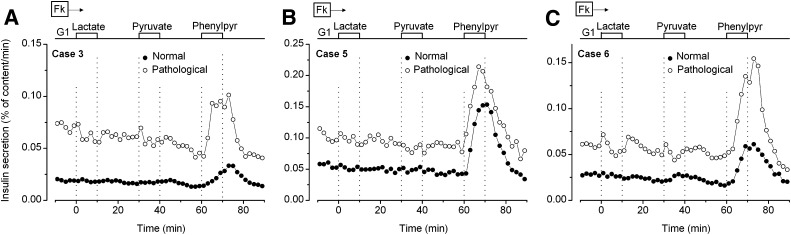
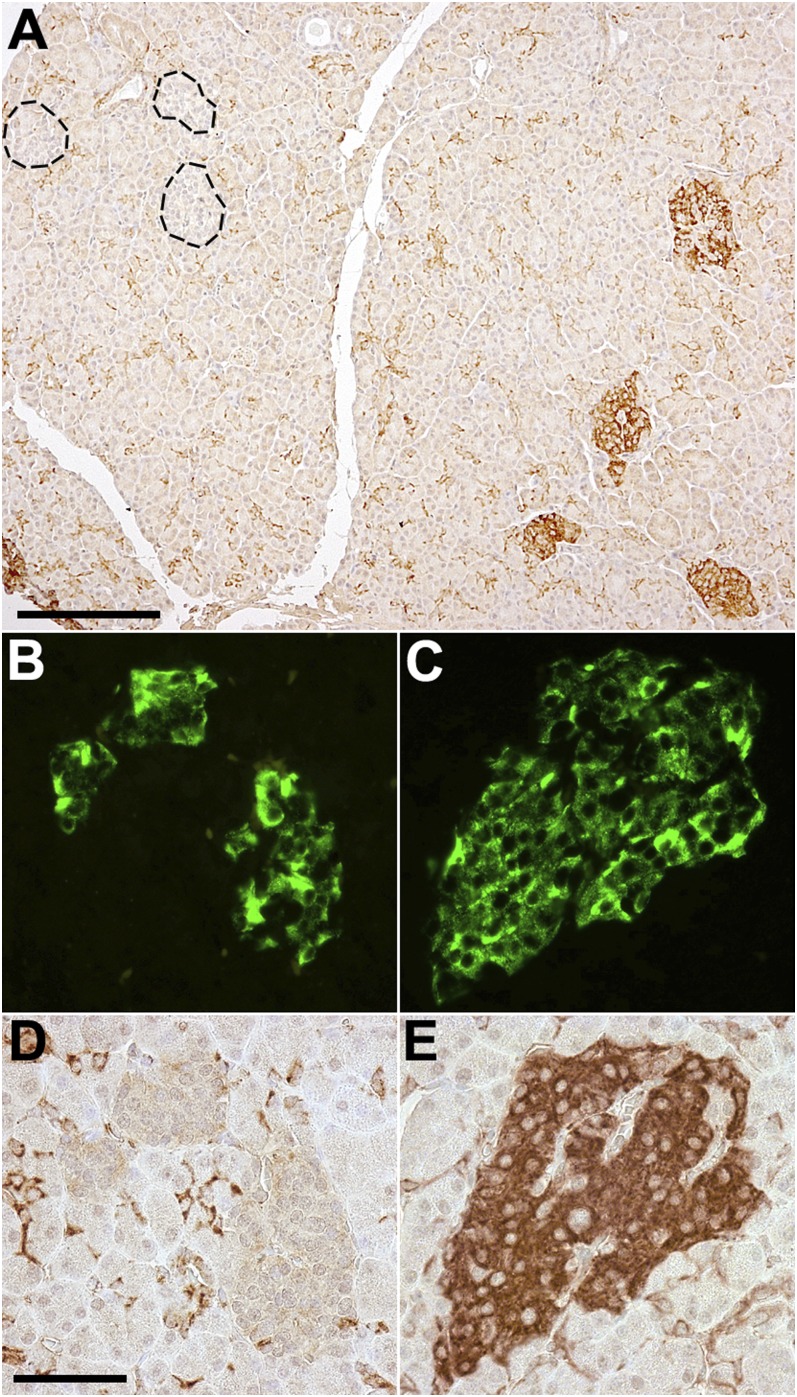
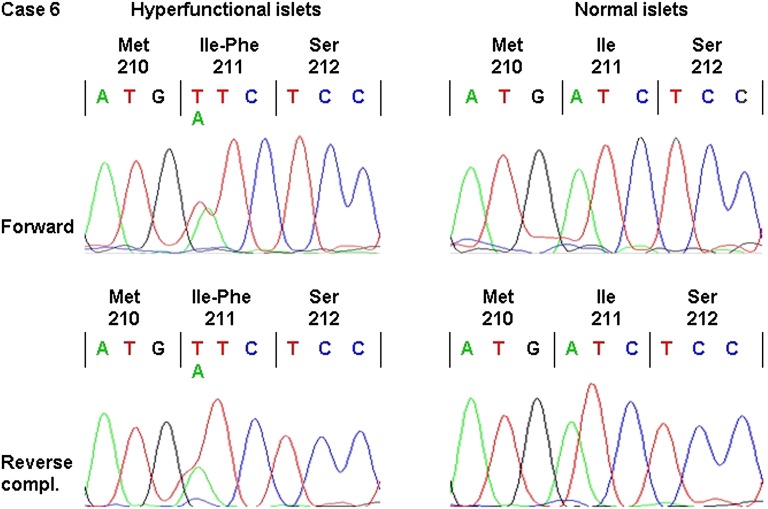
Congenital hyperinsulinism causes persistent hypoglycemia in neonates and infants. Most often, uncontrolled insulin secretion (IS) results from a lack of functional K(ATP) channels in all β-cells or only in β-cells within a resectable focal lesion. In more rare cases, without K(ATP) channel mutations, hyperfunctional islets are confined within few lobules, whereas hypofunctional islets are present throughout the pancreas. They also can be cured by selective partial pancreatectomy; however, unlike those with a K(ATP) focal lesion, they show clinical sensitivity to diazoxide. Here, we characterized in vitro IS by fragments of pathological and adjacent normal pancreas from six such cases. Responses of normal pancreas were unremarkable. In pathological region, IS was elevated at 1 mmol/L and was further increased by 15 mmol/L glucose. Diazoxide suppressed IS and tolbutamide antagonized the inhibition. The most conspicuous anomaly was a large stimulation of IS by 1 mmol/L glucose. In five of six cases, immunohistochemistry revealed undue presence of low-K(m) hexokinase-I in β-cells of hyperfunctional islets only. In one case, an activating mutation of glucokinase (I211F) was found in pathological islets only. Both abnormalities, attributed to somatic genetic events, may account for inappropriate IS at low glucose levels by a subset of β-cells. They represent a novel cause of focal congenital hyperinsulinism.
Figures
Comment in
-
New insights and new conundrums in neonatal hypoglycemia: enigmas wrapped in mystery.Diabetes. 2013 May;62(5):1373-5. doi: 10.2337/db12-1839. Diabetes. 2013. PMID: 23613554 Free PMC article. No abstract available.
References
-
- De León DD, Stanley CA. Mechanisms of Disease: advances in diagnosis and treatment of hyperinsulinism in neonates. Nat Clin Pract Endocrinol Metab 2007;3:57–68 - PubMed
-
- Arnoux JB, de Lonlay P, Ribeiro MJ, et al. Congenital hyperinsulinism. Early Hum Dev 2010;86:287–294 - PubMed
-
- Senniappan S, Shanti B, James C, Hussain K. Hyperinsulinaemic hypoglycaemia: genetic mechanisms, diagnosis and management. J Inherit Metab Dis 2012;35:589–601 - PubMed
-
- Thomas PM, Cote GJ, Wohllk N, et al. Mutations in the sulfonylurea receptor gene in familial persistent hyperinsulinemic hypoglycemia of infancy. Science 1995;268:426–429 - PubMed
-
- Thomas P, Ye Y, Lightner E. Mutation of the pancreatic islet inward rectifier Kir6.2 also leads to familial persistent hyperinsulinemic hypoglycemia of infancy. Hum Mol Genet 1996;5:1809–1812 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
