

Effect of timing of surgery on neurological outcome and survival in metastatic spinal cord compression
- PMID: 23275041
- PMCID: PMC3676569
- DOI: 10.1007/s00586-012-2635-y
Effect of timing of surgery on neurological outcome and survival in metastatic spinal cord compression
Abstract
Purpose: Metastatic spinal cord compression (MSCC) requires expeditious treatment. While there is no ambiguity in the literature about the urgency of care for patients with MSCC, the effect of timing of surgical intervention has not been investigated in detail. The objective of our study was to investigate whether or not the 'timing of surgery' is an important factor in survival and neurological outcome in patients with MSCC.
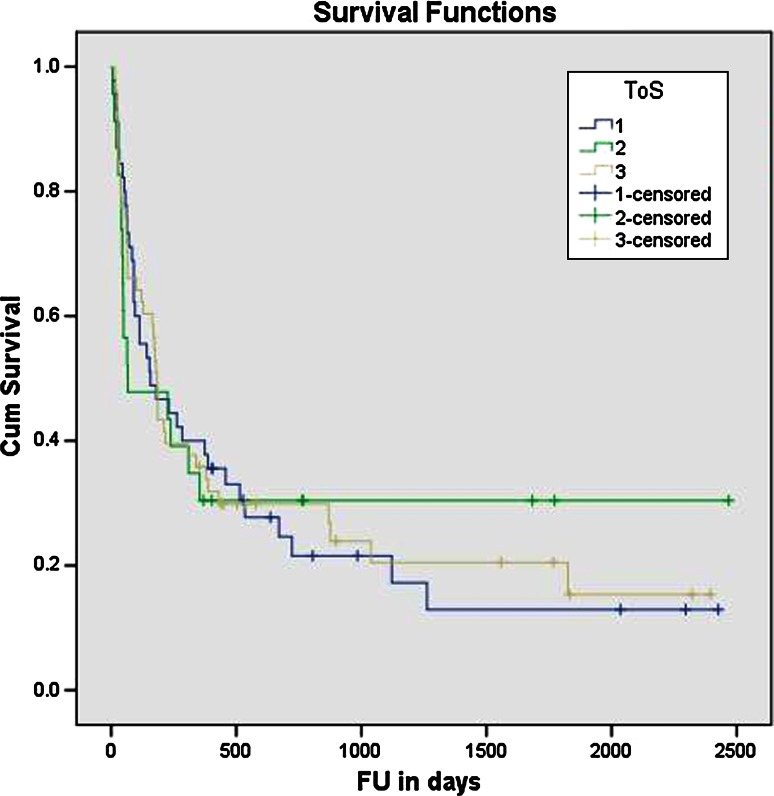
Methods: All patients with MSCC presenting to our unit from October 2005 to March 2010 were included in this study. Patients were divided into three groups-those who underwent surgery within 24 h (Group 1, n = 45), between 24 and 48 h (Group 2, n = 23) and after 48 h (Group 3, n = 53) from acute presentation of neurological symptoms. The outcome measures studied were neurological outcome (change in Frankel grade post-operatively), survival (survival rate and median survival in days), incidence of infection, length of stay and complications.
Results: Patients' age, gender, revised Tokuhashi score, level of spinal metastasis and primary tumour type were not significantly different between the three groups. Greatest improvement in neurology was observed in Group 1, although not significantly when compared against Group 2 (24-48 h; (p = 0.09). When comparisons of neurological outcome were performed for all patients having surgery within 48 h (Groups 1 and 2) versus after 48 h (Group 3), the Frankel grade improvement was significant (p = 0.048) favouring surgery within 48 h of presentation. There was a negative correlation (-0.17) between the delay in surgery and the immediate neurological improvement, suggesting less improvement in those who had delayed surgery. There was no difference in length of hospital stay, incidence of infection, post-operative complications or survival between the groups.
Conclusions: Our results show that surgery should be performed sooner rather than later. Furthermore, earlier surgical treatment within 48 h in patients with MSCC resulted in significantly better neurological outcome. However, the timing of surgery did not influence length of hospital stay, complication rate or patient survival.
Figures
References
-
- Nelson KA, Walsh D, Abdullah O, McDonnell F, Homsi J, Komurcu S, et al. Common complications of advanced cancer. Semin Oncol. 2000;27(1):34–44. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
