

Once-weekly exenatide versus once- or twice-daily insulin detemir: randomized, open-label, clinical trial of efficacy and safety in patients with type 2 diabetes treated with metformin alone or in combination with sulfonylureas
- PMID: 23275363
- PMCID: PMC3631870
- DOI: 10.2337/dc12-1333
Once-weekly exenatide versus once- or twice-daily insulin detemir: randomized, open-label, clinical trial of efficacy and safety in patients with type 2 diabetes treated with metformin alone or in combination with sulfonylureas
Abstract
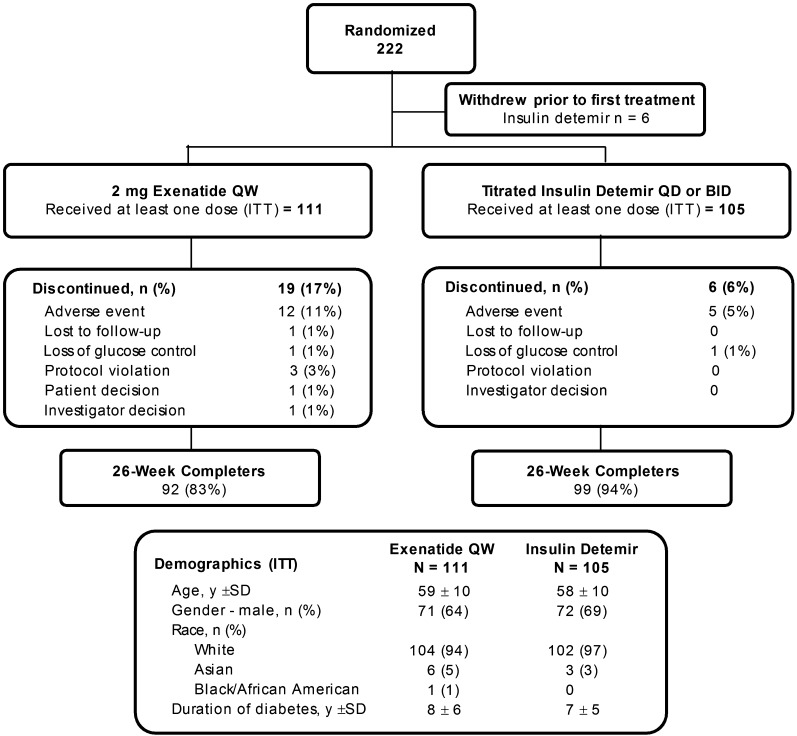
Objective: This multicenter, open-label, parallel-arm study compared the efficacy and safety of exenatide once weekly (EQW) with titrated insulin detemir in patients with type 2 diabetes inadequately controlled with metformin (with or without sulfonylureas).
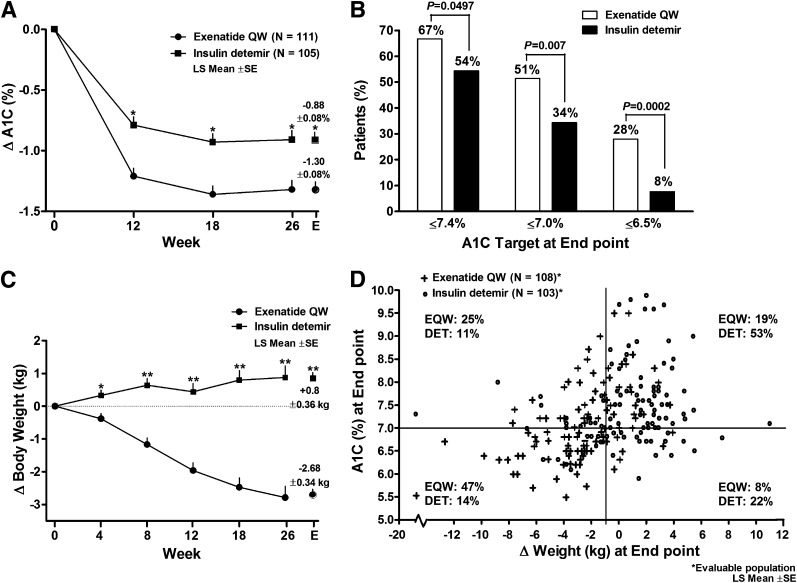
Research design and methods: Patients were randomized to EQW (2 mg) or detemir (once or twice daily, titrated to achieve fasting plasma glucose ≤5.5 mmol/L) for 26 weeks. The primary outcome was proportion of patients achieving A1C ≤7.0% and weight loss ≥1.0 kg at end point, analyzed by means of logistic regression. Secondary outcomes included measures of glycemic control, cardiovascular risk factors, and safety and tolerability.
Results: Of 216 patients (intent-to-treat population), 111 received EQW and 105 received detemir. Overall, 44.1% (95% CI, 34.7-53.9) of EQW-treated patients compared with 11.4% (6.0-19.1) of detemir-treated patients achieved the primary outcome (P < 0.0001). Treatment with EQW resulted in significantly greater reductions than detemir in A1C (least-square mean ± SE, -1.30 ± 0.08% vs. -0.88 ± 0.08%; P < 0.0001) and weight (-2.7 ± 0.3 kg vs. +0.8 ± 0.4 kg; P < 0.0001). Gastrointestinal-related and injection site-related adverse events occurred more frequently with EQW than with detemir. There was no major hypoglycemia in either group. Five (6%) patients in the EQW group and six (7%) patients in the detemir group experienced minor hypoglycemia; only one event occurred without concomitant sulfonylureas (detemir group).
Conclusions: Treatment with EQW resulted in a significantly greater proportion of patients achieving target A1C and weight loss than treatment with detemir, with a low risk of hypoglycemia. These results suggest that EQW is a viable alternative to insulin detemir treatment in patients with type 2 diabetes with inadequate glycemic control using oral antidiabetes drugs.
Figures
References
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2012;55:1577–1596 - PubMed
-
- Rodbard HW, Jellinger PS, Davidson JA, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract 2009;15:540–559 - PubMed
-
- International Diabetes Federation (IDF) Clinical Guidelines Task Force. Global guideline for type 2 diabetes. Brussels: International Diabetes Federation, 2005. Available from http://www.idf.org/webdata/docs/IDF%20GGT2D.pdf Accessed October 26, 2012
-
- NICE clinical guideline 87. Type 2 diabetes: The management of type 2 diabetes. May 2009. Available from http://www.nice.org.uk/nicemedia/live/12165/44320/44320.pdf Accessed October 26, 2012
-
- Bergenstal RM, Wysham C, MacConell L, et al. DURATION-2 Study Group Efficacy and safety of exenatide once weekly versus sitagliptin or pioglitazone as an adjunct to metformin for treatment of type 2 diabetes (DURATION-2): a randomised trial. Lancet 2010;376:431–439 - PubMed
