

Cost-effectiveness of percutaneous coronary intervention with drug eluting stents versus bypass surgery for patients with diabetes mellitus and multivessel coronary artery disease: results from the FREEDOM trial
- PMID: 23277307
- PMCID: PMC3603704
- DOI: 10.1161/CIRCULATIONAHA.112.147488
Cost-effectiveness of percutaneous coronary intervention with drug eluting stents versus bypass surgery for patients with diabetes mellitus and multivessel coronary artery disease: results from the FREEDOM trial
Abstract
Background: Studies from the balloon angioplasty and bare metal stent eras have demonstrated that coronary artery bypass grafting (CABG) is cost-effective compared with percutaneous coronary intervention (PCI) for patients undergoing multivessel coronary revascularization-particularly among patients with complex coronary artery disease or diabetes mellitus. Whether these results apply in the drug-eluting stent (DES) era is unknown.
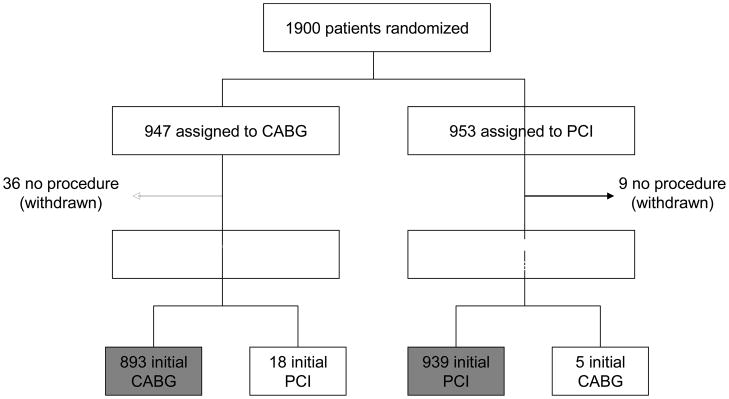
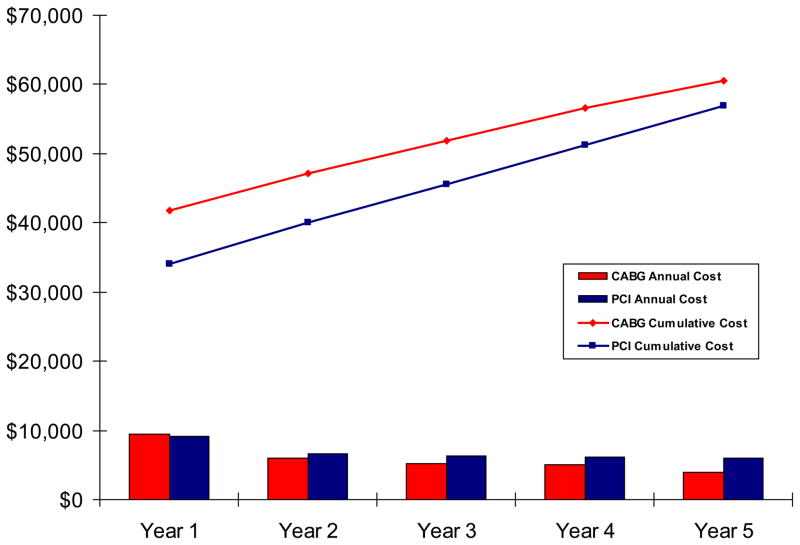
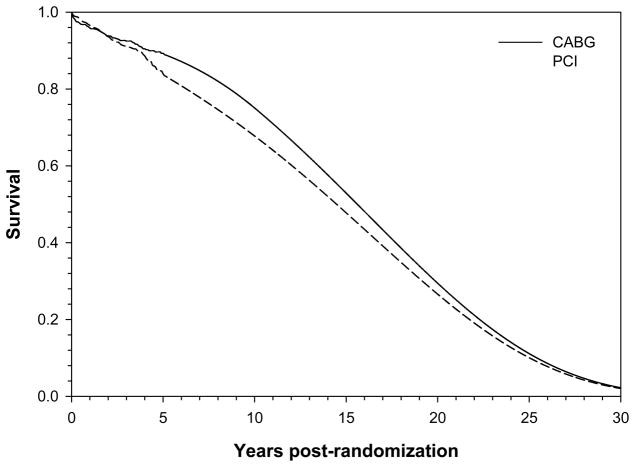
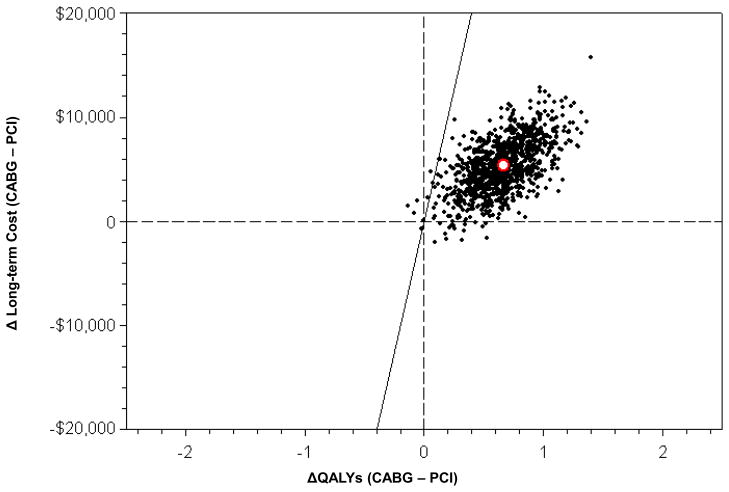
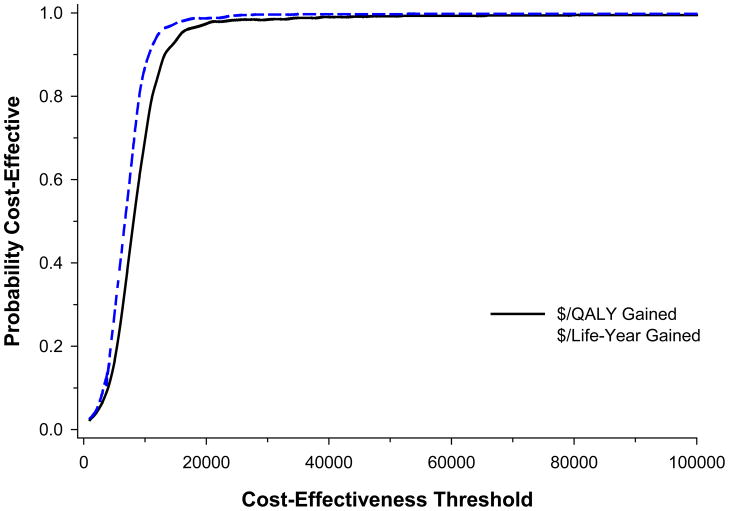
Methods and results: Between 2005 and 2010, 1900 patients with diabetes mellitus and multivessel coronary artery disease were randomized to PCI with DES (DES-PCI; n=953) or CABG (n=947). Costs were assessed from the perspective of the U.S. health care system. Health state utilities were assessed using the EuroQOL 5 dimension 3 level questionnaire. A patient-level microsimulation model based on U.S. life-tables and in-trial results was used to estimate lifetime cost-effectiveness. Although initial procedural costs were lower for CABG, total costs for the index hospitalization were $8622 higher per patient. Over the next 5 years, follow-up costs were higher with PCI, owing to more frequent repeat revascularization and higher outpatient medication costs. Nonetheless, cumulative 5-year costs remained $3641 higher per patient with CABG. Although there were only modest gains in survival with CABG during the trial period, when the in-trial results were extended to a lifetime horizon, CABG was projected to be economically attractive relative to DES-PCI, with substantial gains in both life expectancy and quality-adjusted life expectancy and incremental cost-effectiveness ratios <$10 000 per life-year or quality-adjusted life-year gained across a broad range of assumptions regarding the effect of CABG on post-trial survival and costs.
Conclusions: Despite higher initial costs, CABG is a highly cost-effective revascularization strategy compared with DES-PCI for patients with diabetes mellitus and multivessel coronary artery disease.
Clinical trial registration: URL: http://www.clinical-trials.gov. Unique identifier: NCT00086450.
Conflict of interest statement
Figures
Comment in
-
Effectiveness is the key to cost-effectiveness.Circulation. 2013 Feb 19;127(7):764-5. doi: 10.1161/CIRCULATIONAHA.113.000639. Circulation. 2013. PMID: 23429894 No abstract available.
References
-
- The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med. 1996;335:217–225. - PubMed
-
- Hlatky MA, Rogers WJ, Johnstone I, Boothroyd D, Brooks MM, Pitt B, Reeder G, Ryan T, Smith H, Whitlow P, Wiens R, Mark DB. Medical care costs and quality of life after randomization to coronary angioplasty or coronary bypass surgery. Bypass Angioplasty Revascularization Investigation (BARI) Investigators. N Engl J Med. 1997;336:92–99. - PubMed
-
- King SB, 3rd, Kosinski AS, Guyton RA, Lembo NJ, Weintraub WS. Eight-year mortality in the emory angioplasty versus surgery trial (east) J Am Coll Cardiol. 2000;35:1116–1121. - PubMed
-
- Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, Stahle E, Feldman TE, van den Brand M, Bass EJ, Van Dyck N, Leadley K, Dawkins KD, Mohr FW. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961–972. - PubMed
-
- Serruys PW, Ong AT, van Herwerden LA, Sousa JE, Jatene A, Bonnier JJ, Schonberger JP, Buller N, Bonser R, Disco C, Backx B, Hugenholtz PG, Firth BG, Unger F. Five-year outcomes after coronary stenting versus bypass surgery for the treatment of multivessel disease: The final analysis of the arterial revascularization therapies study (ARTS) randomized trial. J Am Coll Cardiol. 2005;46:575–581. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
