

Systematic review and meta-analysis of combination therapy with cholinesterase inhibitors and memantine in Alzheimer's disease and other dementias
- PMID: 23277787
- PMCID: PMC3522458
- DOI: 10.1159/000343479
Systematic review and meta-analysis of combination therapy with cholinesterase inhibitors and memantine in Alzheimer's disease and other dementias
Abstract
Background: N-methyl-D-aspartic acid antagonists (memantine) and cholinesterase inhibitors (ChEIs) are the only two approved classes of drugs to treat dementia; this paper explores the evidence for using these two treatments in combination.
Objective: To determine the efficacy and safety of using combination therapy with memantine and a ChEI to treat dementia in comparison to monotherapy with either memantine or a ChEI.
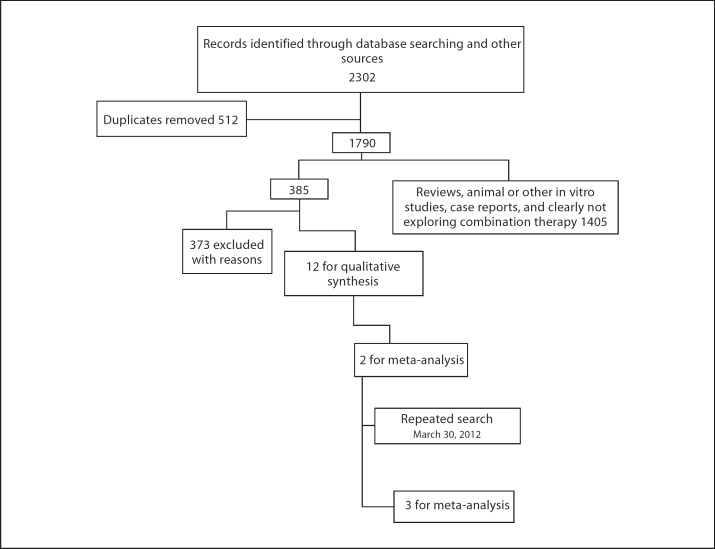
Methods: In March 2012, we systematically searched MEDLINE/PubMed, EMBASE, Cochrane library, and grey literature databases. All study types were included, except for case series or reports, which looked at combination therapy versus monotherapy in various dementing disorders. Data was pooled for blinded randomized controlled trials (RCTs) only; mean differences and standardized mean differences were used to determine effect sizes.
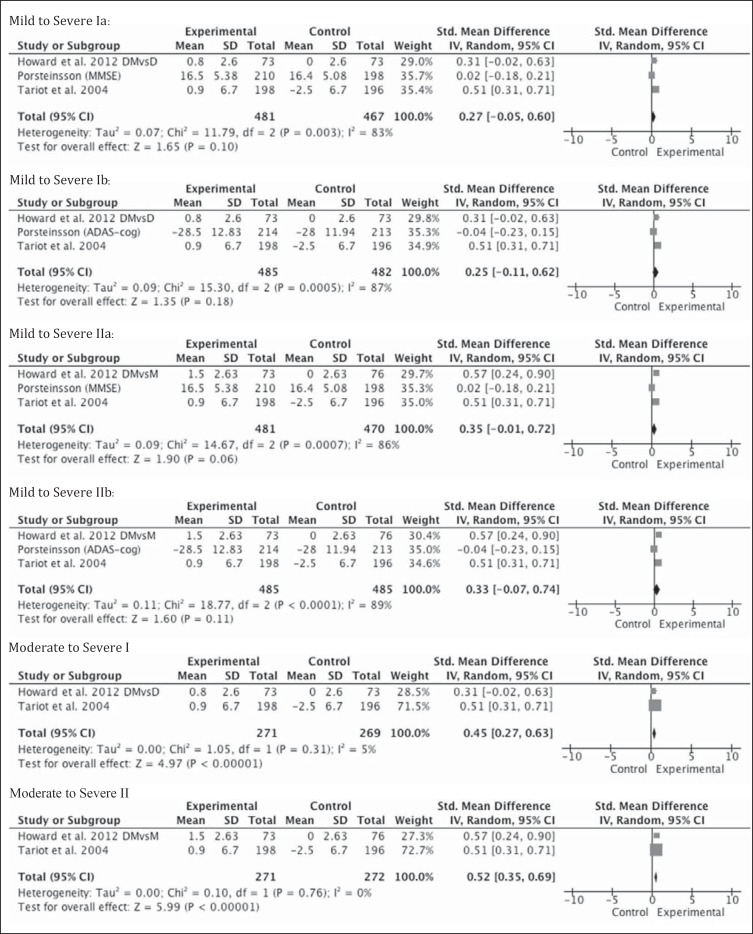
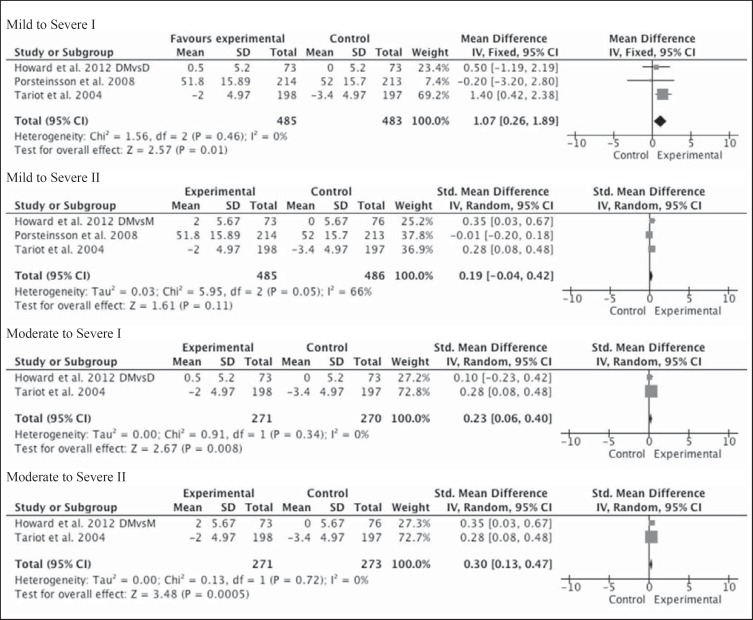
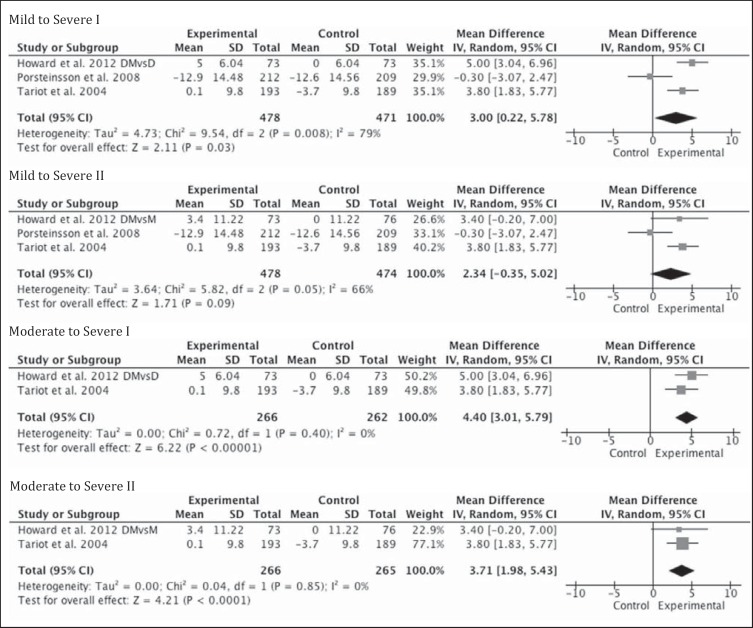
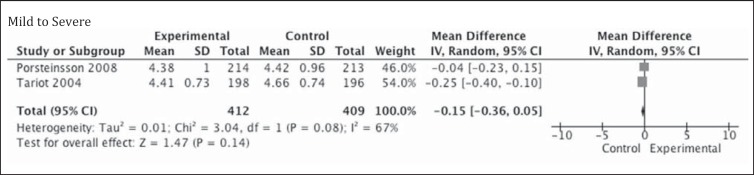
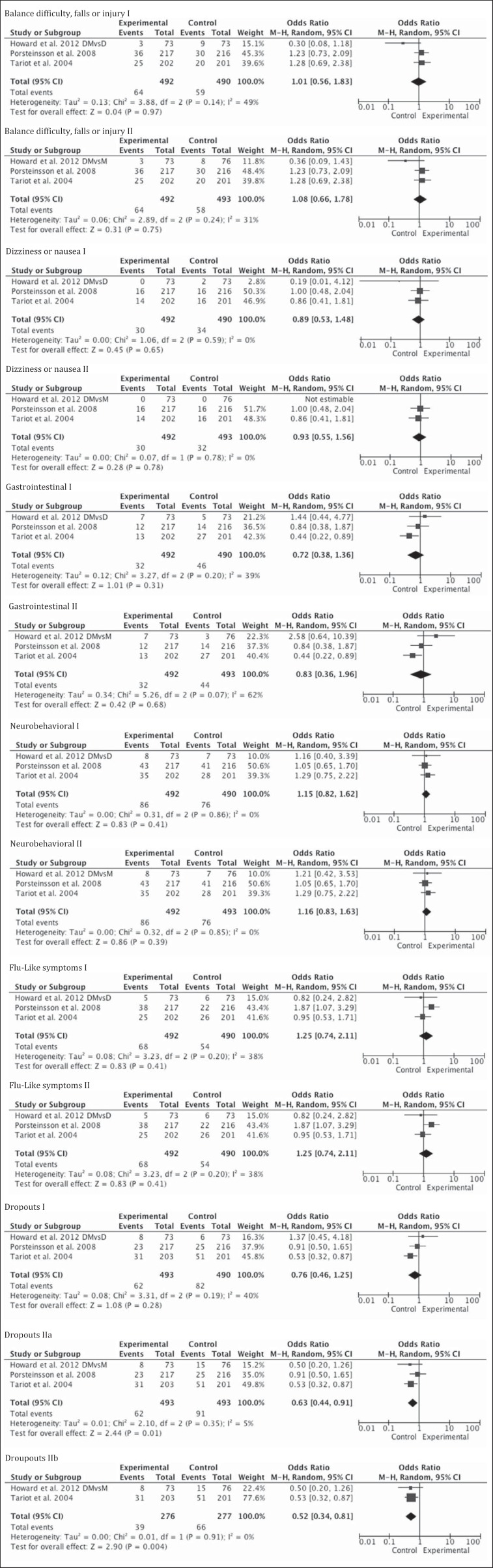
Results: Thirteen studies were included in this review; 3 were blinded RCTs, with a total of 971 Alzheimer's disease (AD) patients, which were included into the meta-analysis. No papers were found that primarily addressed combination therapy in other dementias. In the meta-analysis, small but statistically significant effect sizes were seen in favor of combination therapy among patients with moderate to severe AD on the scales of cognition (0.45-0.52; p < 0.0001), scales of functional outcomes (0.23-0.3; p < 0.01), and the neuropsychiatric inventory (3.7-4.4; p < 0.0001). Among the open-label studies, 3 out of 6 suggested benefits, as did the 4 included cohort studies. However, the high risk of bias encountered in the latter two study designs limits deducing any conclusions about benefit.
Conclusion: Although there were statistically significant changes in favor of combination therapy in moderate to severe AD, heterogeneity in scales and patient characteristics exists. However, it is unclear if clinically significant outcomes can be achieved using the combination therapy. More studies are required before a recommendation for combination therapy can be made.
Keywords: Alzheimer; Cholinesterase inhibitors; Combination treatment; Dementia; Dementia therapy; Memantine; Side effects.
Figures
References
-
- The Alzheimer Society Rising Tide: The Impact of Dementia on Canadian Society. 2009.
-
- Wimo A, Winblad B. Economic aspects on drug therapy of dementia. Curr Pharm Des. 2004;10:295–301. - PubMed
-
- Wimo A, Winblad B, Jonsson L. An estimate of the total worldwide societal costs of dementia in 2005. Alzheimers Dement. 2007;3:81–91. - PubMed
-
- Wimo A, Winblad B, Jonsson L. The worldwide societal costs of dementia: estimates for 2009. Alzheimers Dement. 2010;6:98–103. - PubMed
-
- Barca ML, Engedal K, Laks J, Selbaek G. Quality of life among elderly patients with dementia in institutions. Dement Geriatr Cogn Disord. 2011;31:435–442. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
