

Ratio of leukotriene e(4) to exhaled nitric oxide and the therapeutic response in children with exercise-induced bronchoconstriction
- PMID: 23277875
- PMCID: PMC3529225
- DOI: 10.4168/aair.2013.5.1.26
Ratio of leukotriene e(4) to exhaled nitric oxide and the therapeutic response in children with exercise-induced bronchoconstriction
Abstract
Purpose: This study assessed the association between the ratio of leukotriene E(4) (LTE(4)) to fractional exhaled nitric oxide (FE(NO)) in the response of children with exercise-induced bronchoconstriction (EIB) enrolled in a therapeutic trial with montelukast or inhaled corticosteroid (fluticasone propionate [FP]).
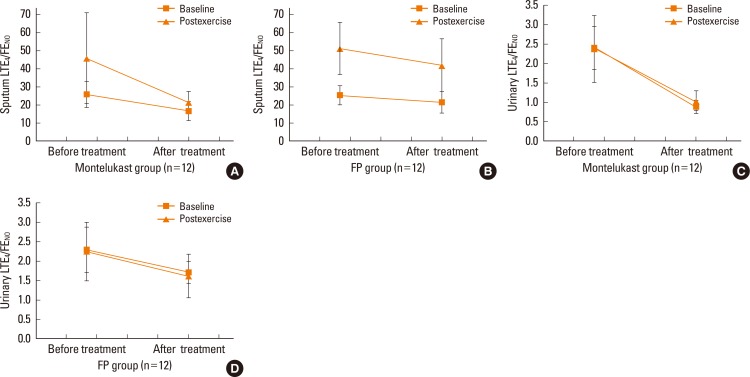
Methods: Children aged 6 to 18 years with EIB were randomized in a 4-week, placebo-controlled, double-blinded trial with montelukast or FP. Before and after treatment, treadmill exercise challenges were performed. The LTE(4) levels in the induced sputum and urine and the FE(NO) levels were measured in subjects before and 30 minutes after the exercise challenges. The same tests were conducted after treatment.
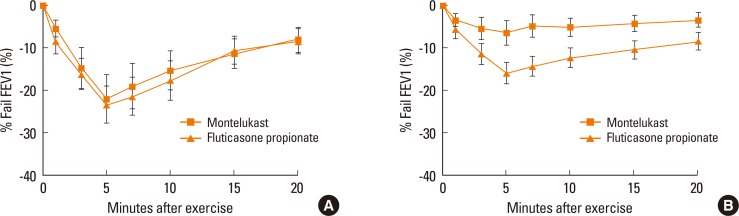
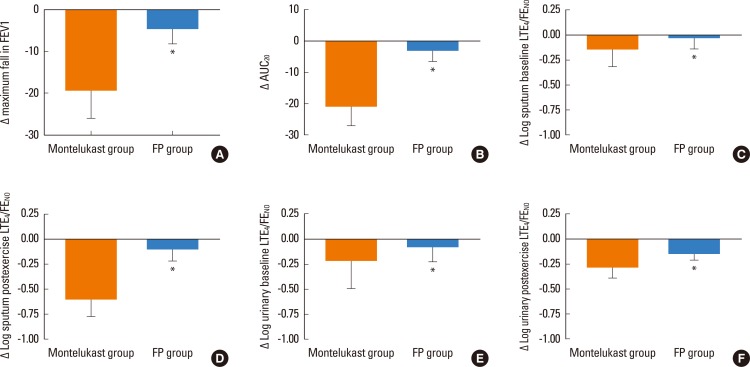
Results: A total of 24 patients completed the study: 12 in the montelukast group and 12 in FP group. Both study groups displayed a similar postexercise maximum decrease in forced expiratory volume in one second (FEV1) before treatment as well as after treatment. However, there were significant differences in the magnitude of change between the two (Δ; -18.38±14.53% vs. -4.67±8.12% for the montelukast and FP groups, respectively; P=0.021). The Δ logarithmic sputum baseline and postexercise LTE(4)/FE(NO) ratio were significantly lower in the montelukast group than in the FP group (baseline; -0.09±0.21 vs. -0.024±0.03, P=0.045; postexercise, -0.61±0.33 vs. -0.11±0.28, P=0.023).
Conclusions: These data indicate that the efficacy of montelukast for preventing a maximum decrease in FEV1 after exercise is significantly higher than that of FP, and the high LTE(4)/FE(NO) ratio is associated with a greater response to montelukast than to FP for EIB therapy. These results suggest that LTE(4) may play an important role in EIB.
Keywords: Exercise-induced bronchoconstriction; fractional exhaled nitric oxide; inhaled corticosteroid; leukotriene E4; montelukast.
Conflict of interest statement
There are no financial or other issues that might lead to conflict of interest.
Figures
References
-
- Cabral AL, Conceição GM, Fonseca-Guedes CH, Martins MA. Exercise-induced bronchospasm in children: effects of asthma severity. Am J Respir Crit Care Med. 1999;159:1819–1823. - PubMed
-
- Joos GF, O'Connor B, Anderson SD, Chung F, Cockcroft DW, Dahlén B, DiMaria G, Foresi A, Hargreave FE, Holgate ST, Inman M, Lötvall J, Magnussen H, Polosa R, Postma DS, Riedler J ERS Task Force. Indirect airway challenges. Eur Respir J. 2003;21:1050–1068. - PubMed
-
- Holgate ST, Lemanske RF, Jr, O'Byrne PM, Kakumanu S, Busse WW. Asthma pathogenesis. In: Adkinson NF, Yunginger JW, Busse WW, Bochner BS, Holgate ST, Simon FE, editors. Middleton's allergy: principles and practice. 7th ed. Philadelphia: Mosby; 2009. p. 893.
-
- O'Sullivan S, Roquet A, Dahlén B, Larsen F, Eklund A, Kumlin M, O'Byrne PM, Dahlén SE. Evidence for mast cell activation during exercise-induced bronchoconstriction. Eur Respir J. 1998;12:345–350. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
