

The gastrointestinal manifestations of telomere-mediated disease
- PMID: 23279657
- PMCID: PMC3602337
- DOI: 10.1111/acel.12041
The gastrointestinal manifestations of telomere-mediated disease
Abstract
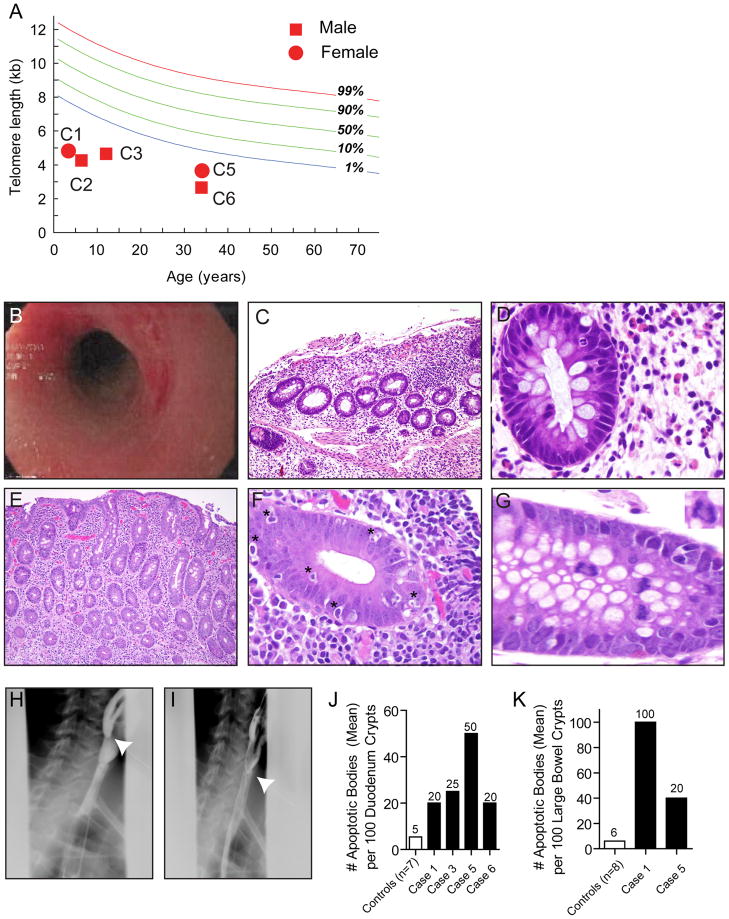
Defects in telomere maintenance genes cause pathological telomere shortening, and manifest in syndromes which have prominent phenotypes in tissues of high turnover: the skin and bone marrow. Because the gastrointestinal (GI) epithelium is highly proliferative, we sought to determine whether telomere syndromes cause GI disease, and to define its prevalence, spectrum, and natural history. We queried subjects in the Johns Hopkins Telomere Syndrome Registry for evidence of luminal GI disease. In sixteen percent of Registry subjects (6 of 38), there was a history of significant GI pathology, and 43 additional cases were identified in the literature. Esophageal stenosis, enteropathy, and enterocolitis were the recurrent findings. In the intestinal mucosa, there was striking villous atrophy, extensive apoptosis, and anaphase bridging pointing to regenerative defects in the epithelial compartment. GI disease was often the first and most severe manifestation of telomere disease in young children. These findings indicate that telomere dysfunction disrupts the epithelial integrity in the human GI tract manifesting in recognizable disease processes. A high index of suspicion should facilitate diagnosis and management.
© 2012 The Authors Aging Cell © 2012 Blackwell Publishing Ltd/Anatomical Society of Great Britain and Ireland.
Conflict of interest statement
Dr. Califano is the Director of Research of the Milton J. Dance Head and Neck Endowment. The terms of this arrangement are being managed by the Johns Hopkins University in accordance with its conflict of interest policies. The other authors have no relevant financial conflict of interest to declare.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
