

An aggregated analysis of hormonal factors and endometrial cancer risk by parity
- PMID: 23280123
- PMCID: PMC3744666
- DOI: 10.1002/cncr.27909
An aggregated analysis of hormonal factors and endometrial cancer risk by parity
Abstract
Background: Nulliparity is associated with an increased risk of endometrial cancer. It is less clear whether nulliparity modifies the association between other established hormone-related risk factors. The proportion of nulliparous women has increased since the mid-1970s, but most individual studies to date have been too small to test the hypothesis that endometrial cancer risk factors may be associated more strongly with risk among nulliparous women compared with parous women.
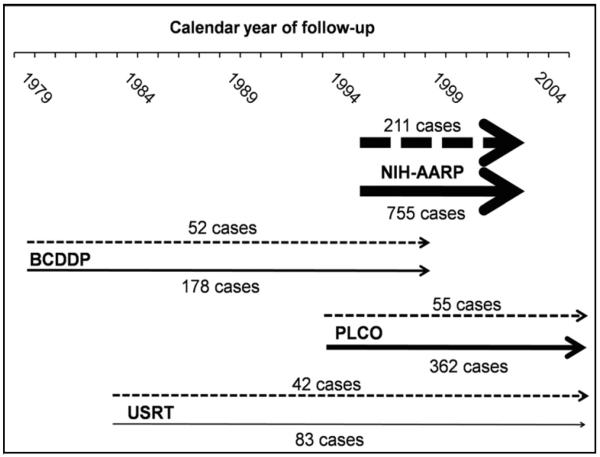
Methods: Data were aggregated on 26,936 postmenopausal, Caucasian, nulliparous women (360 endometrial cancers) and 146,583 postmenopausal, Caucasian, parous women (1378 endometrial cancers) from 4 US prospective studies (1979-2006). Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated in stratified analyses.
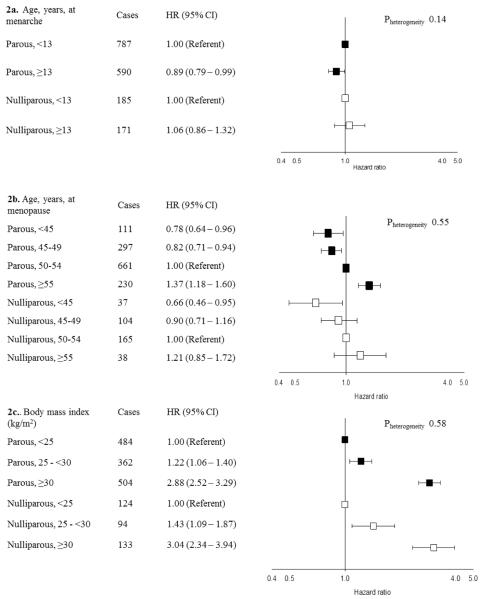
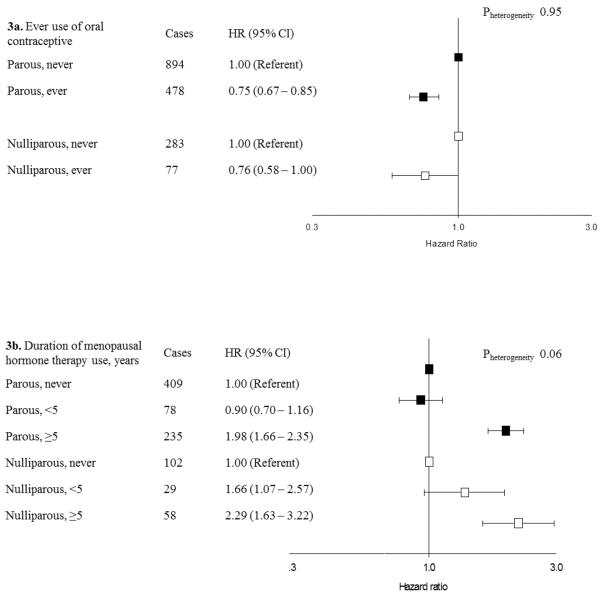
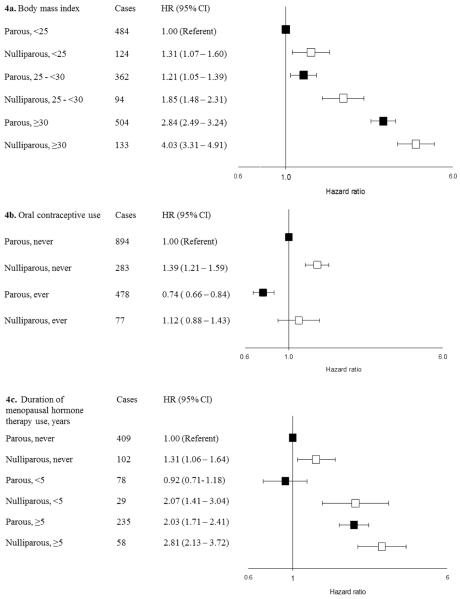
Results: The risk of endometrial cancer was higher among nulliparous women than among parous women, as expected (nulliparous vs parous: HR, 1.42; 95% CI, 1.26-1.60). Stratified associations between endometrial cancer and hormone-related risk factors did not differ between nulliparous versus parous women: For both groups, oral contraceptives and earlier menopause were associated with reduced risk. The highest HRs were for obesity: A body mass index ≥30 kg/m(2) (vs <25 kg/m(2) ) increased the risk of endometrial cancer 3-fold among nulliparous women (HR, 3.04; 95% CI, 2.34-3.94) and parous women (HR, 2.88; 95% CI, 2.52-3.29).
Conclusions: The results from this large, pooled analysis of data from 4 large prospective studies suggested that nulliparity does not modify the risks of endometrial cancer associated with established hormone-related risk factors.
Copyright © 2012 American Cancer Society.
Figures
Similar articles
-
Hormone-related risk factors and postmenopausal breast cancer among nulliparous versus parous women: An aggregated study.Am J Epidemiol. 2011 Mar 1;173(5):509-17. doi: 10.1093/aje/kwq404. Epub 2011 Jan 25. Am J Epidemiol. 2011. PMID: 21266505 Free PMC article.
-
Parity and time interval since childbirth influence survival in endometrial cancer patients.Int J Gynecol Cancer. 2009 May;19(4):665-9. doi: 10.1111/IGC.0b013e3181a3e1bf. Int J Gynecol Cancer. 2009. PMID: 19509568
-
Infertility and incident endometrial cancer risk: a pooled analysis from the epidemiology of endometrial cancer consortium (E2C2).Br J Cancer. 2015 Mar 3;112(5):925-33. doi: 10.1038/bjc.2015.24. Epub 2015 Feb 17. Br J Cancer. 2015. PMID: 25688738 Free PMC article.
-
The role of pregnancy, perinatal factors and hormones in maternal cancer risk: a review of the evidence.J Intern Med. 2018 May;283(5):430-445. doi: 10.1111/joim.12747. Epub 2018 Mar 25. J Intern Med. 2018. PMID: 29476569 Free PMC article. Review.
-
Weighing the evidence on the pill and breast cancer.Fam Plann Perspect. 1989 Mar-Apr;21(2):89-92. Fam Plann Perspect. 1989. PMID: 2653859 Review.
Cited by
-
Female Hormonal Factors and the Risk of Endometrial Cancer in Lynch Syndrome.JAMA. 2015 Jul 7;314(1):61-71. doi: 10.1001/jama.2015.6789. JAMA. 2015. PMID: 26151267 Free PMC article.
-
Cancer Incidence by Occupation in Korea: Longitudinal Analysis of a Nationwide Cohort.Saf Health Work. 2020 Mar;11(1):41-49. doi: 10.1016/j.shaw.2019.12.004. Epub 2019 Dec 31. Saf Health Work. 2020. PMID: 32206373 Free PMC article.
-
Intra-Individual Consistency in Endocrine Profiles Across Successive Pregnancies.J Clin Endocrinol Metab. 2015 Dec;100(12):4637-47. doi: 10.1210/jc.2015-2620. Epub 2015 Oct 20. J Clin Endocrinol Metab. 2015. PMID: 26485218 Free PMC article.
-
Parity Correlates with the Timing of Developing Endometrial Cancer, But Not Subtype of Endometrial Cancer.J Cancer. 2015 Sep 3;6(11):1087-92. doi: 10.7150/jca.12736. eCollection 2015. J Cancer. 2015. PMID: 26516355 Free PMC article.
-
Expression of Selected Epithelial-Mesenchymal Transition Transcription Factors in Endometrial Cancer.Biomed Res Int. 2020 Dec 29;2020:4584250. doi: 10.1155/2020/4584250. eCollection 2020. Biomed Res Int. 2020. PMID: 33457409 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
