

Urine proteomics for discovery of improved diagnostic markers of Kawasaki disease
- PMID: 23281308
- PMCID: PMC3569638
- DOI: 10.1002/emmm.201201494
Urine proteomics for discovery of improved diagnostic markers of Kawasaki disease
Abstract
Kawasaki disease (KD) is a systemic vasculitis of unknown etiology. Absence of definitive diagnostic markers limits the accuracy of clinical evaluations of suspected KD with significant increases in morbidity. In turn, incomplete understanding of its molecular pathogenesis hinders the identification of rational targets needed to improve therapy. We used high-accuracy mass spectrometry proteomics to analyse over 2000 unique proteins in clinical urine specimens of patients with KD. We discovered that urine proteomes of patients with KD, but not those with mimicking conditions, were enriched for markers of cellular injury such as filamin and talin, immune regulators such as complement regulator CSMD3, immune pattern recognition receptor muclin, and immune cytokine protease meprin A. Significant elevations of filamin C and meprin A were detected in both the serum and urine in two independent cohorts of patients with KD, comprised of a total of 236 patients. Meprin A and filamin C exhibited superior diagnostic performance as compared to currently used markers of disease in a blinded case-control study of 107 patients with suspected KD, with receiver operating characteristic areas under the curve of 0.98 (95% confidence intervals [CI] of 0.97-1 and 0.95-1, respectively). Notably, meprin A was enriched in the coronary artery lesions of a mouse model of KD. In all, urine proteome profiles revealed novel candidate molecular markers of KD, including filamin C and meprin A that exhibit excellent diagnostic performance. These disease markers may improve the diagnostic accuracy of clinical evaluations of children with suspected KD, lead to the identification of novel therapeutic targets, and allow the development of a biological classification of Kawasaki disease.
Copyright © 2013 The Authors. Published by John Wiley and Sons, Ltd on behalf of EMBO.
Figures
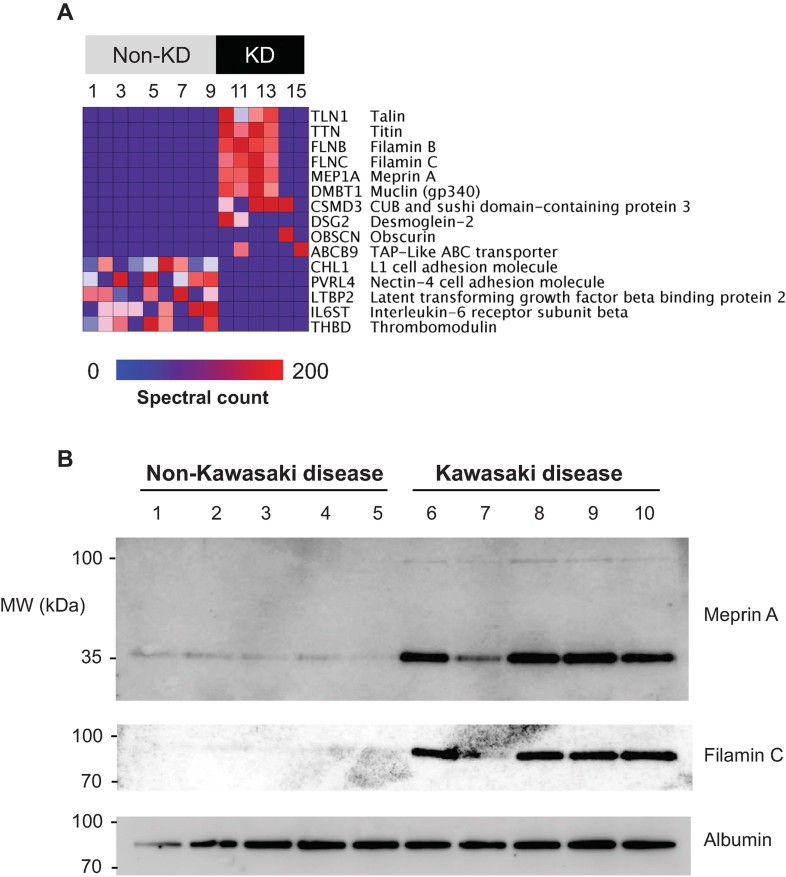
Heatmap of the 15 individual urinary proteomes (columns) showing the results of Bayesian analysis of the top 10 proteins (rows) that are detected in patients with KD as compared to those without. The top 5 proteins that are detected in patients without KD as compared to those with KD are shown for comparison. Blue-to-red colour gradient represents the number of MS/MS spectra (spectral count) that corresponds to urinary protein abundance.
Western immunoblot analysis of meprin A and filamin C in urine, demonstrating enrichment of meprin A and filamin C in the urine of patients with KD as compared to patients without KD. Note that meprin A and filamin C are detected predominantly as partial-length isoforms, with apparent molecular weights of 35 and 80 kDa, respectively. Albumin serves as the loading control.
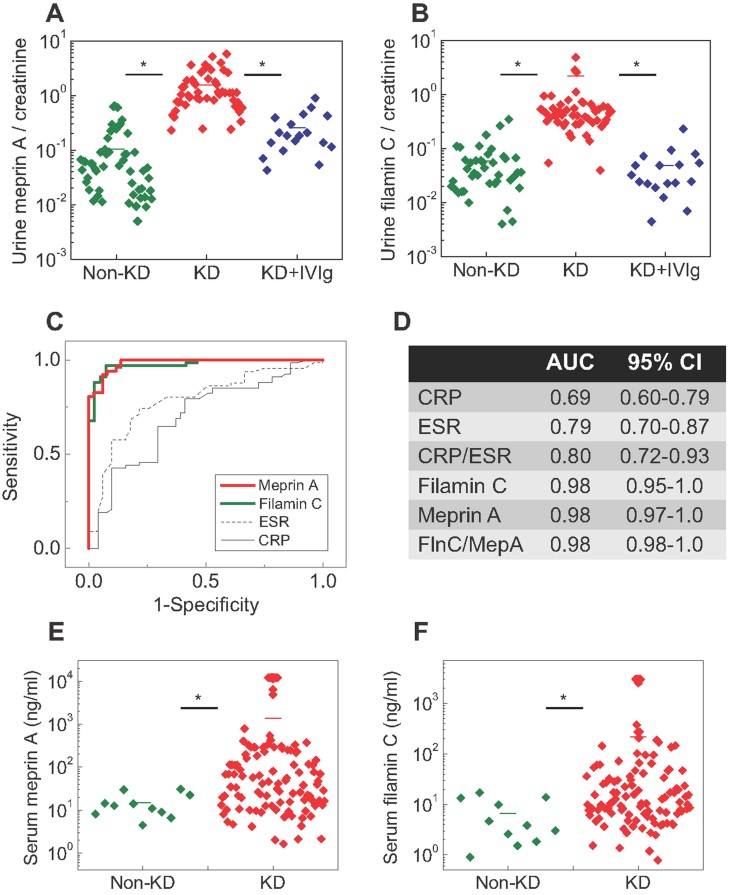
A,B. otplots of urine concentrations measured using specific ELISAs of meprin A (A) and filamin C (B) in a blinded case-control study of patients suspected of KD, demonstrating significantly elevated concentrations of meprin A and filamin C in patients with KD (red) as compared to those with non-KD conditions (green) and patients with KD upon receiving IVIg treatment (blue). p = 2.0E−8 and 1.3E−17 for filamin C and meprin A, respectively. Horizontal bars represent means for each comparison group. Note the logarithmic scale of meprin A and filamin C concentrations.
C. Receiver operating characteristics of urine meprin A (red) and filamin C (green), as compared to common markers, ESR (dashed black) and blood CRP (solid black).
D. Receiver operating characteristic area under the curve (AUC) values and their 95% confidence intervals (CI) for the measured diagnostic markers.
E,F. Dotplots of serum concentrations measured using specific ELISAs of meprin A (E) and filamin C (F) in patients with KD (red) as compared to patients with non-KD mimicking conditions (green). p = 1.2E−7 and 3.9E−4 for filamin C and meprin A, respectively.
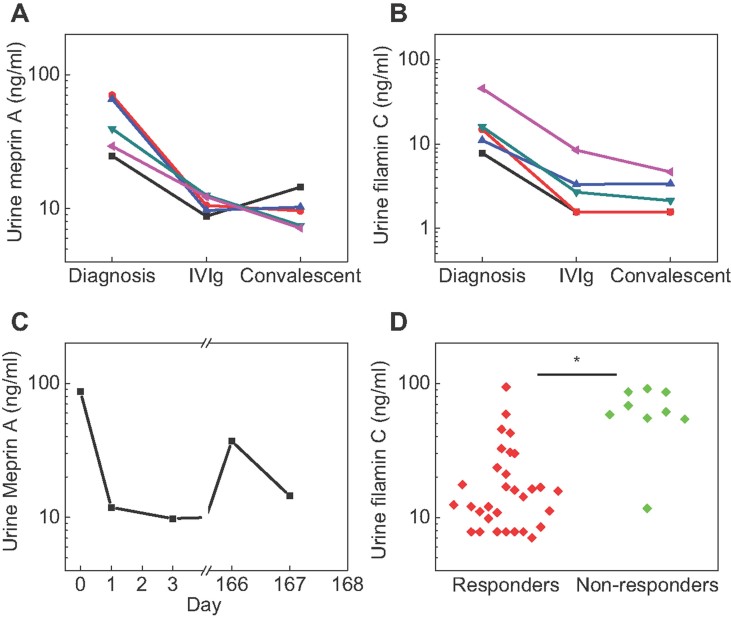
A,B. Urine meprin A (A) and filamin C (B) levels in five patients with KD, as measured in matched specimens collected at diagnosis, 24–48 h after treatment, and 1 month after complete clinical response.
C. Urine meprin A level in one patient who experienced recurrence of KD 5.5 months after initial presentation.
D. Scatter plot showing urine filamin C levels in patients who responded to initial therapy (red, responders) versus those who required repeat treatment (green, non-responders). p = 0.0015.
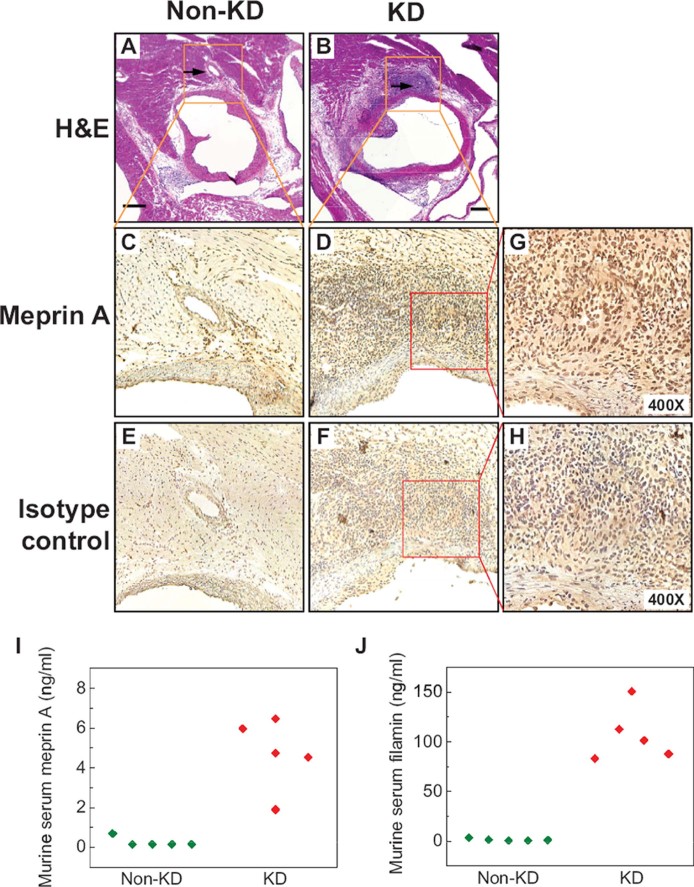
A,B. Micrographs of hematoxylin and eosin-stained sections of the aortic root and coronary arteries of control (A) and LCWE-injected mice (B) demonstrating severe aortitis with intimal proliferation leading to concentric obstruction in the LCWE-injected but not control animals. Arrows point to the normal (A) and diseased (B) coronary arteries.
C,D. Micrographs of meprin A immunohistochemistry-stained inset areas of the sections of coronary arteries demonstrating enrichment of meprin A in the mononuclear infiltrates of coronary arteries in LCWE-injected (D) but not control (C) animals.
E,F. Micrographs of isotype control-stained sections of coronary arteries in LCWE-injected (F) and control (E) mice.
G,H. High-magnification micrographs of the inset areas of meprin A (G) and isotype control-strained (H) sections of the coronary arteries in LCWE-injected mice.
I,J. Serum levels of meprin A (I) and filamin (J) are elevated in the LCWE-injected (red) as compared to control (green) mice. Scale bar is 250 µM.
References
-
- Bangert I, Tumulka F, Abele R. The lysosomal polypeptide transporter TAPL: more than a housekeeping factor. Biol Chem. 2011;392:61–66. - PubMed
-
- Bond JS, Matters GL, Banerjee S, Dusheck RE. Meprin metalloprotease expression and regulation in kidney, intestine, urinary tract infections and cancer. FEBS Lett. 2005;579:3317–3322. - PubMed
-
- Bonnemann CG, Thompson TG, van der Ven PF, Goebel HH, Warlo I, Vollmers B, Reimann J, Herms J, Gautel M, Takada F, et al. Filamin C accumulation is a strong but nonspecific immunohistochemical marker of core formation in muscle. J Neurol Sci. 2003;206:71–78. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K08 CA160660/CA/NCI NIH HHS/United States
- M01 RR002172/RR/NCRR NIH HHS/United States
- U01 HL068269/HL/NHLBI NIH HHS/United States
- U01 HL068290/HL/NHLBI NIH HHS/United States
- U01 HL068288/HL/NHLBI NIH HHS/United States
- U01 HL068281/HL/NHLBI NIH HHS/United States
- U01 HL068270/HL/NHLBI NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- UL1 RR 025758/RR/NCRR NIH HHS/United States
- K08CA160660/CA/NCI NIH HHS/United States
- U01 HL068292/HL/NHLBI NIH HHS/United States
- P30 HD018655/HD/NICHD NIH HHS/United States
- RR 02172/RR/NCRR NIH HHS/United States
- U01 HL068279/HL/NHLBI NIH HHS/United States
- U01 HL068285/HL/NHLBI NIH HHS/United States
- U01 HL068285,/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
