

Review
doi: 10.1172/JCI62874.
Epub 2013 Jan 2.
Myocardial ischemia-reperfusion injury: a neglected therapeutic target
Affiliations
- PMID: 23281415
- PMCID: PMC3533275
- DOI: 10.1172/JCI62874
Item in Clipboard
Review
Myocardial ischemia-reperfusion injury: a neglected therapeutic target
J Clin Invest.
2013 Jan.
Abstract
Acute myocardial infarction (MI) is a major cause of death and disability worldwide. In patients with MI, the treatment of choice for reducing acute myocardial ischemic injury and limiting MI size is timely and effective myocardial reperfusion using either thombolytic therapy or primary percutaneous coronary intervention (PPCI). However, the process of reperfusion can itself induce cardiomyocyte death, known as myocardial reperfusion injury, for which there is still no effective therapy. A number of new therapeutic strategies currently under investigation for preventing myocardial reperfusion injury have the potential to improve clinical outcomes in patients with acute MI treated with PPCI.
Figures
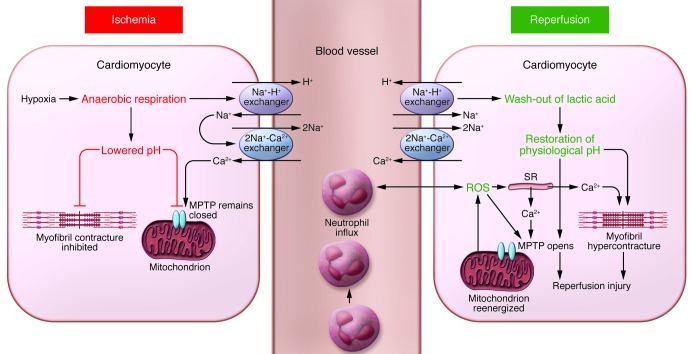
During acute myocardial ischemia, the absence of oxygen switches cell metabolism to anaerobic respiration, resulting in the production of lactate and a drop in intracellular pH. This induces the Na+-H+ exchanger to extrude H+ and results in intracellular Na+ overload, which activates the 2Na+-Ca2+ exchanger to function in reverse to extrude Na+ and leads to intracellular Ca2+ overload. The Na+-K+ ATPase ceases to function in ischemia, exacerbating intracellular Na+ overload. The acidic conditions during ischemia prevent the opening of the MPTP and cardiomyocyte hypercontracture at this time. During reperfusion, the electron transport chain is reactivated, generating ROS. Other sources of ROS include xanthine oxidase (endothelial cells) and NADPH oxidase (neutrophils). ROS mediate myocardial reperfusion injury by inducing the opening of the MPTP, acting as a neutrophil chemoattractant, and mediating dysfunction of the sarcoplasmic reticulum (SR). This contributes to intracellular Ca2+ overload and damages the cell membrane by lipid peroxidation, inducing enzyme denaturation and causing direct oxidative damage to DNA. Reperfusion and reactivation of the Na+-H+ exchanger result in washout of lactic acid, resulting in the rapid restoration of physiological pH, which releases the inhibitory effect on MPTP opening and cardiomyocyte contracture. The restoration of the mitochondrial membrane potential drives calcium into the mitochondria, which can also induce MPTP opening. Several hours after the onset of myocardial reperfusion, neutrophils accumulate in the infarcted myocardial tissue in response to the release of the chemoattractants ROS, cytokines, and activated complement.
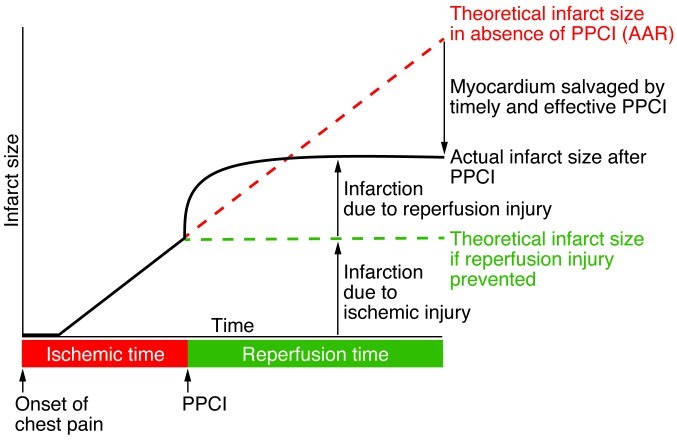
The black solid line depicts the individual contributions to final MI size of acute myocardial ischemic injury and of myocardial reperfusion injury. The green dashed line depicts the theoretical MI size following PPCI based on acute myocardial ischemia alone in the absence of myocardial reperfusion injury. The red dashed line depicts the theoretical MI size based on acute myocardial ischemia alone in the absence of PPCI. The presence of myocardial reperfusion injury attenuates the benefit of PPCI in terms of the reduction of MI size. Therefore, the administration of a therapeutic strategy as an adjunct to PPCI that is capable of reducing myocardial reperfusion injury would result in a smaller MI size (as depicted by the green dashed line) and take advantage of full benefits of myocardial reperfusion. Figure modified from Cardiovascular Research (93).
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
