

Critical factors in cut-out complication after Gamma Nail treatment of proximal femoral fractures
- PMID: 23281775
- PMCID: PMC3543839
- DOI: 10.1186/1471-2474-14-1
Critical factors in cut-out complication after Gamma Nail treatment of proximal femoral fractures
Abstract
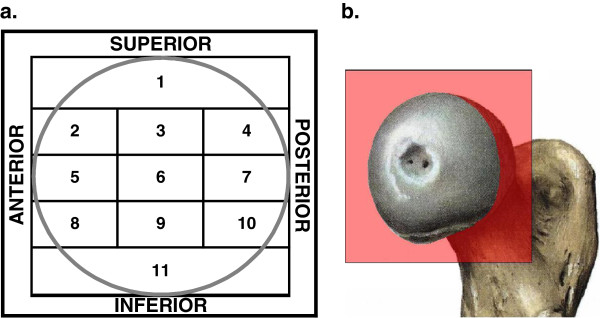
Background: The most common mechanical failure in the internal fixation of trochanteric hip fractures is the cut-out of the sliding screw through the femoral head. Several factors that influence this complication have been suggested, but there is no consensus as to the relative importance of each factor. The purpose of this study was to analyse the cut-out complication with respect to the following variables: patients' age, fracture type, fracture reduction, implant positioning and implant design.
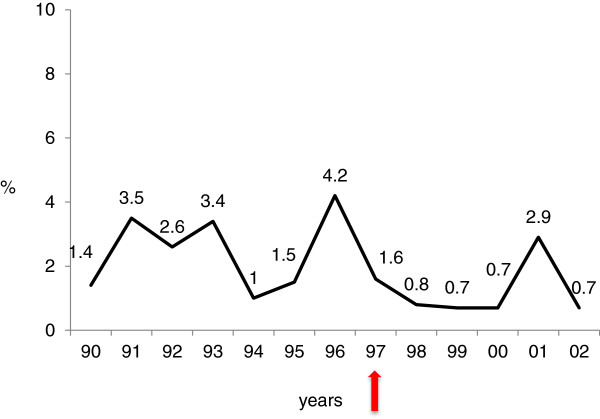
Methods: 3066 consecutive patients were treated for trochanteric fractures with Gamma Nails between 1990 and 2002 at the Centre de Traumatologie et de l'Orthopedie (CTO), Strasbourg, France. Cut-out complications were identified by reviewing all available case notes and radiographs. Subsequently, the data were analysed by a single reviewer (AJB) with focus on the studied factors.
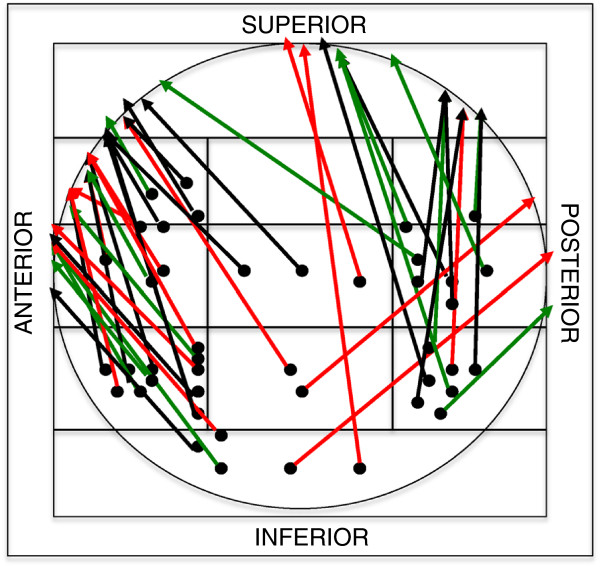
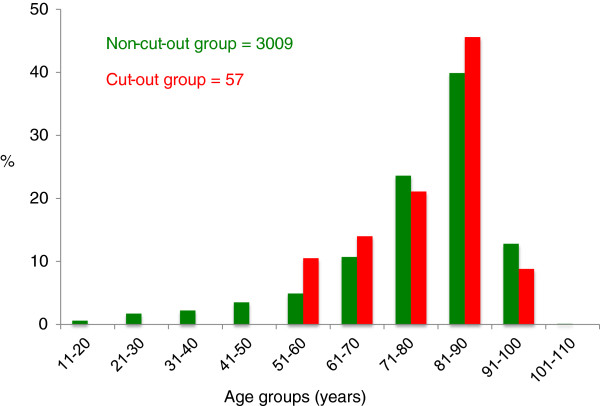
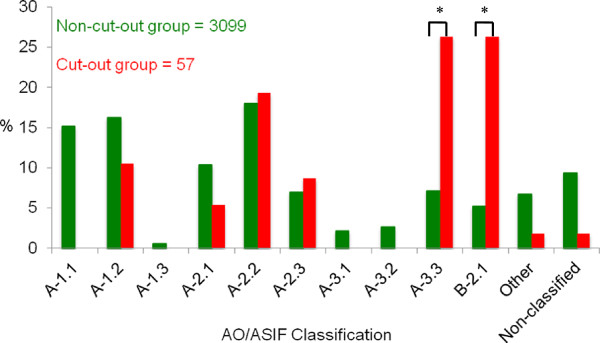
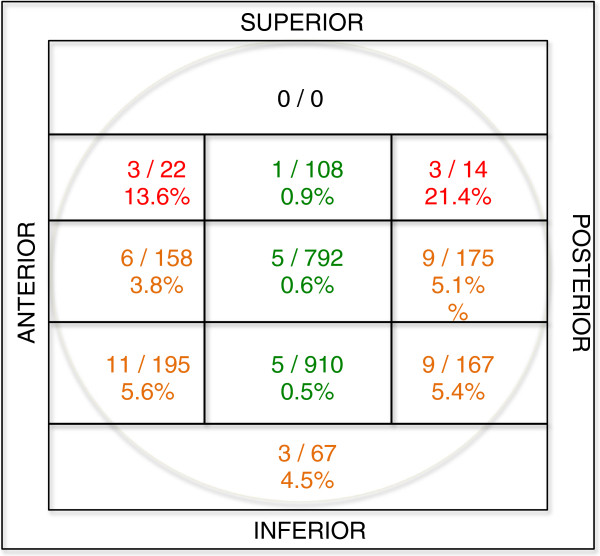
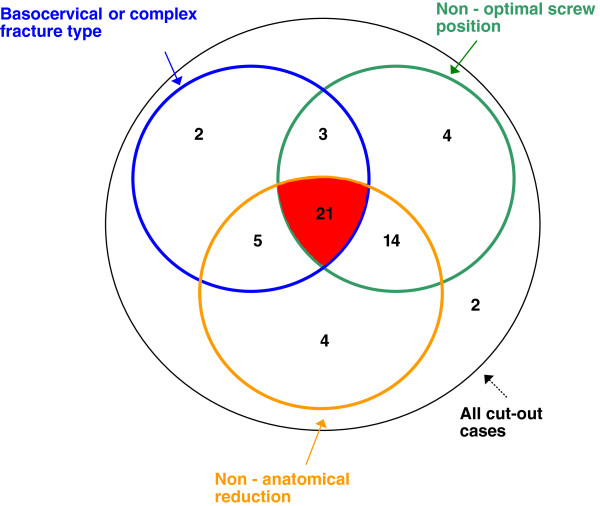
Results: Seventy-one cut-out complications were found (2.3%) of the 3066 trochanteric fractures. Cut-out failure associated with avascular head necrosis, pathologic fracture, deep infection or secondary to prior failure of other implants were excluded from the study (14 cases). The remaining 57 cases (1.85%, median age 82.6, 79% females) were believed to have a biomechanical explanation for the cut-out failure. 41 patients had a basicervical or complex fracture type. A majority of cut-outs (43 hips, 75%) had a combination of the critical factors studied; non-anatomical reduction, non-optimal lag screw position and the characteristic fracture pattern found.
Conclusions: The primary cut-out rate of 1.85% was low compared with the literature. A typical cut-out complication in our study is represented by an unstable fracture involving the trochanteric and cervical regions or the combination of both, non-anatomical reduction and non-optimal screw position. Surgeons confronted with proximal femoral fractures should carefully scrutinize preoperative radiographs to assess the primary fracture geometry and fracture classification. To reduce the risk of a cut-out it is important to achieve both anatomical reduction and optimal lag screw position as these are the only two factors that can be controlled by the surgeon.
Figures
References
-
- Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995;77(7):1058–1064. - PubMed
-
- Nordin S, Zulkifli O, Faisham WI. Mechanical failure of Dynamic Hip Screw (DHS) fixation in intertrochanteric fracture of the femur. Med J Malaysia. 2001;56(Suppl D):12–17. - PubMed
-
- Davis TR, Sher JL, Horsman A, Simpson M, Porter BB, Checketts RG. Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone Joint Surg Br. 1990;72(1):26–31. - PubMed
-
- Utrilla AL, Reig JS, Munoz FM, Tufanisco CB. Trochanteric gamma nail and compression hip screw for trochanteric fractures: a randomized, prospective, comparative study in 210 elderly patients with a new design of the gamma nail. J Orthop Trauma. 2005;19(4):229–233. doi: 10.1097/01.bot.0000151819.95075.ad. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
