

Angioedema
- PMID: 23282406
- PMCID: PMC3651192
- DOI: 10.1097/WOX.0b013e31817aecbe
Angioedema
Abstract
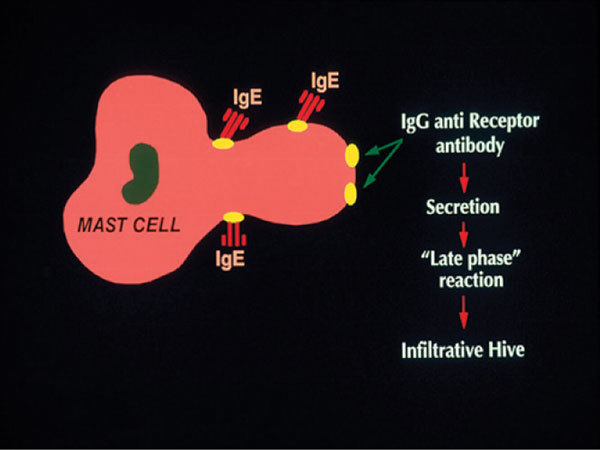
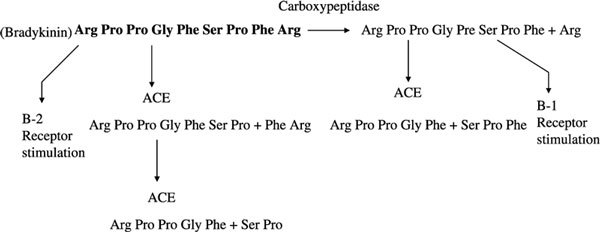
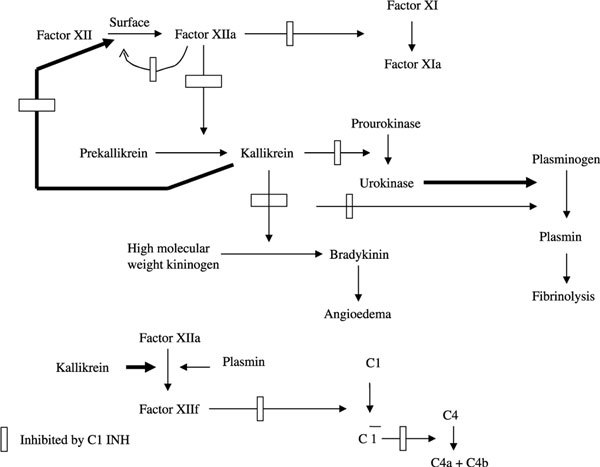
Angioedema can be caused by either mast cell degranulation or activation of the kallikrein-kinin cascade. In the former case, angioedema can be caused by allergic reactions caused by immunoglobulin E (IgE)-mediated hypersensitivity to foods or drugs that can also result in acute urticaria or a more generalized anaphylactic reaction. Nonsteroidal anti-inflammatory drugs (cyclooxygenase 1 inhibitors, in particular) may cause angioedema with or without urticaria, and leukotrienes may have a particular role as a mediator of the swelling. Reactions to contrast agents resemble allergy with basophil and mast cell degranulation in the absence of specific IgE antibody and can be generalized, that is, anaphylactoid. Angioedema accompanies chronic urticaria in 40% of patients, and approximately half have an autoimmune mechanism in which there is IgG antibody directed to the subunit of the IgE receptor (40%) or to IgE itself (5%-10%). Bradykinin is the mediator of angioedema in hereditary angioedema types I and II (C1 inhibitor [INH] deficiency) and the newly described type III disorder some of which are caused bya mutation involving factor XII. Acquired C1 INH deficiency presents in a similar fashion to the hereditary disorder and is due either toC1 INH depletion by circulating immune complexes or to an IgG antibody directed to C1 INH. Although each of these causes excessive bradykinin formation because of activation of the plasma bradykinin-forming pathway, the angioedema due to angiotensin-converting enzyme inhibitors is caused by excessive bradykinin levels due to inhibition of bradykinin degradation. Idiopathic angioedema (ie, pathogenesis unknown) may be histaminergic, that is, caused by mast cell degranulation with histamine release, or nonhistaminergic. The mediator pathways in the latter case are yet to be defined. A minority may be associated with the same autoantibodies associated with chronic urticaria. Angioedema that is likely to be life threatening (laryngeal edema or tongue/pharyngeal edema that obstructs the airway) is seen in anaphylactic/anaphylactoid reactions and the disorders mediated by bradykinin.
Figures

References
-
- Black A. In: Urticaria and Angioedema. Greaves M, Kaplan A, editor. New York, NY: Marcel Dekker; 2004. Physical urticaria and cholinergic urticaria; pp. 171–214.
LinkOut - more resources
Full Text Sources
