

HIV pathogenesis: dynamics and genetics of viral populations and infected cells
- PMID: 23284080
- PMCID: PMC3530041
- DOI: 10.1101/cshperspect.a012526
HIV pathogenesis: dynamics and genetics of viral populations and infected cells
Abstract
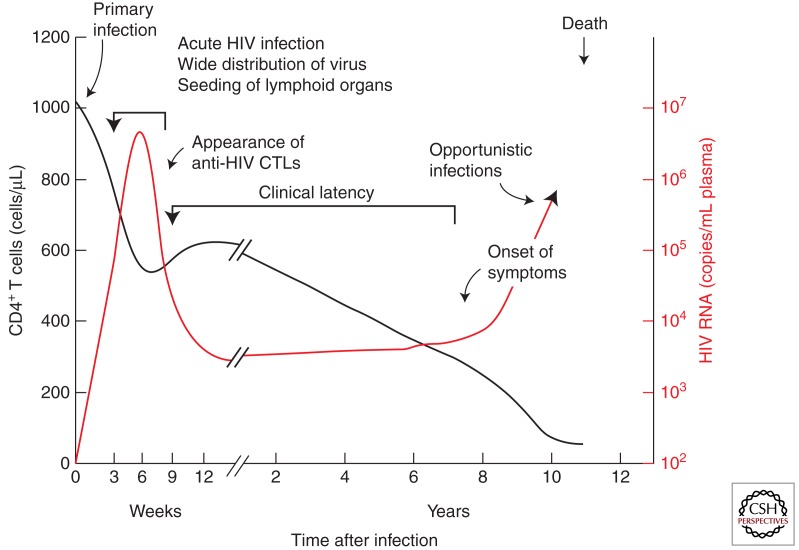
In the absence of treatment, HIV-1 infection, usually starting with a single virion, leads inexorably to a catastrophic decline in the numbers of CD4(+) T cells and to AIDS, characterized by numerous opportunistic infections as well as other symptoms, including dementia and wasting. In the 30 years since the AIDS pandemic came to our attention, we have learned a remarkable amount about HIV-1, the responsible virus--the molecular details about how it functions and interacts with the host cell, its evolution within the host, and the countermeasures it has evolved to overcome host defenses against viral infection. Despite these advances, we remain remarkably ignorant about how HIV-1 infection leads to disease and the death of the human host. In this brief article, we introduce and discuss important lessons that we have learned by examining the dynamics of viral populations and infected cells. These studies have revealed important features of the virus-host interaction that now form the basis of our understanding of the importance and consequence of ongoing viral replication during HIV-1 infection.
Figures
References
-
- Bailey JR, Sedaghat AR, Kieffer T, Brennan T, Lee PK, Wind-Rotolo M, Haggerty CM, Kamireddi AR, Liu Y, Lee J, et al. 2006. Residual human immunodeficiency virus type 1 viremia in some patients on antiretroviral therapy is dominated by a small number of invariant clones rarely found in circulating CD4+ T cells. J Virol 80: 6441–6457 - PMC - PubMed
-
- Buzon MJ, Massanella M, Llibre JM, Esteve A, Dahl V, Puertas MC, Gatell JM, Domingo P, Paredes R, Sharkey M, et al. 2011. HIV-1 replication and immune dynamics are affected by raltegravir intensification of HAART-suppressed subjects. Nat Med 16: 460–465 - PubMed
-
- Chersich MF, Gray GE 2005. Progress and emerging challenges in preventing mother-to-child transmission. Curr Infect Dis Rep 7: 393–400 - PubMed
-
- Chun TW, Carruth L, Finzi D, Shen X, DiGiuseppe JA, Taylor H, Hermankova M, Chadwick K, Margolick J, Quinn TC, et al. 1997. Quantification of latent tissue reservoirs and total body viral load in HIV-1 infection. Nature 387: 183–188 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials