

The efficacy and tolerability of 'polypills': meta-analysis of randomised controlled trials
- PMID: 23284906
- PMCID: PMC3526586
- DOI: 10.1371/journal.pone.0052145
The efficacy and tolerability of 'polypills': meta-analysis of randomised controlled trials
Abstract
Background: To assess the blood pressure and lipid-lowering efficacy and tolerability of 'polypills' used in cardiovascular disease prevention trials.
Methodology/principal findings: Systematic review and meta-analysis.
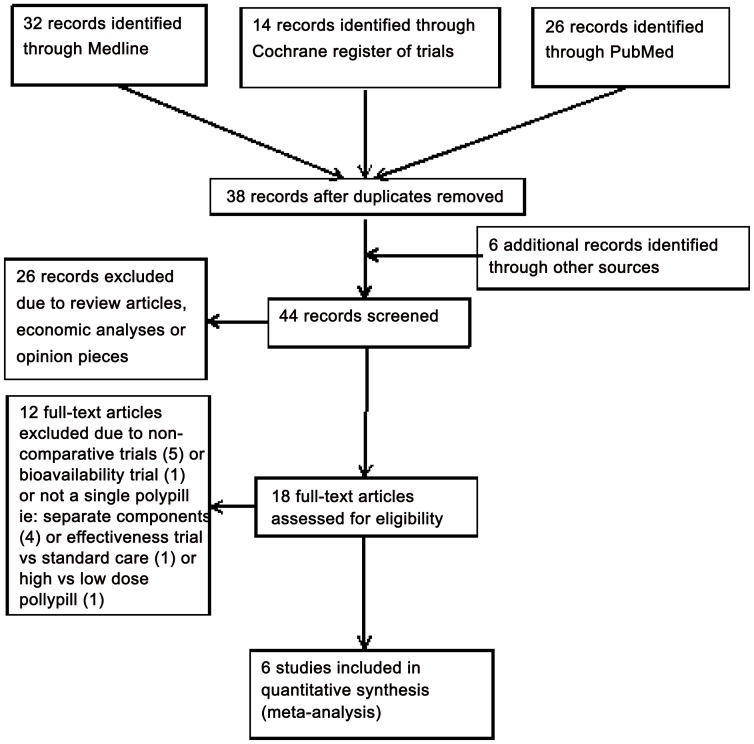
Search strategy: The Cochrane Central Register of Controlled Trials, Medline, and PubMed databases were searched for eligible trials. Study inclusion criteria: Randomised controlled trials of at least six weeks duration, which compared a 'polypill' (that included at least one anti-hypertensive and one lipid-lowering medication) with a placebo (or one active component).
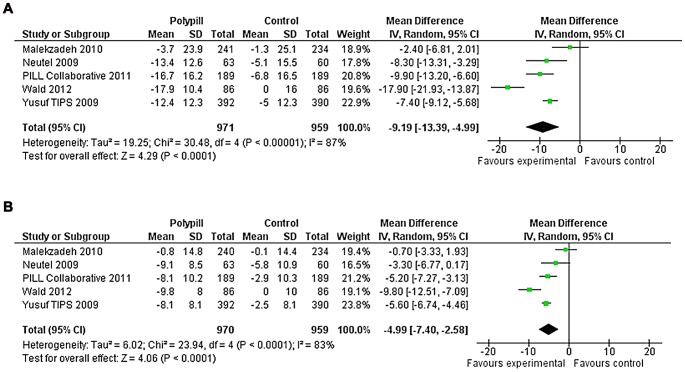
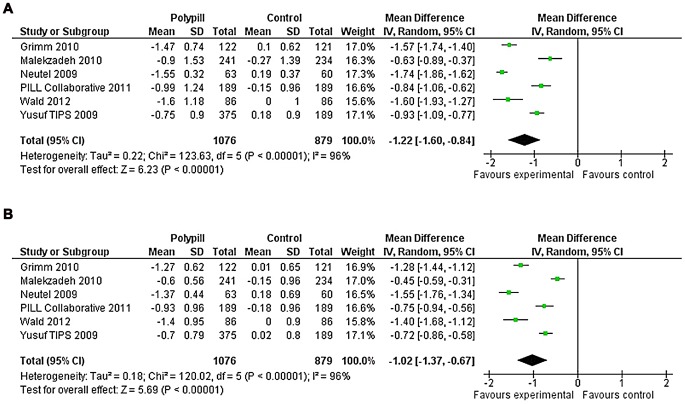
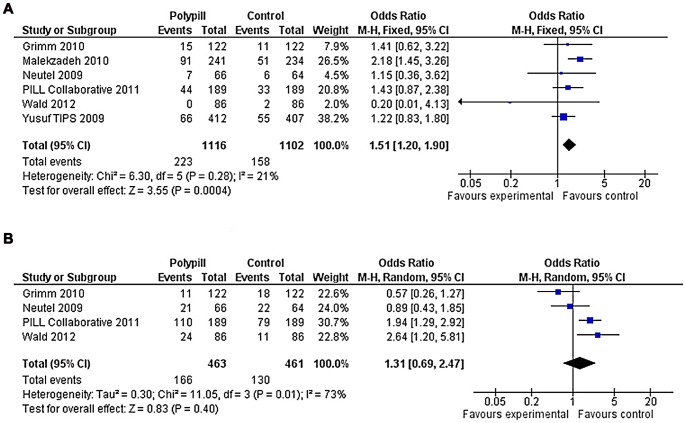
Outcome measures: Change from baseline in systolic and diastolic blood pressures, and total and LDL-cholesterol; discontinuation of study medication and reported adverse effects. Of 44 potentially eligible studies, six trials (including 2,218 patients without previous cardiovascular disease) fulfilled the inclusion criteria. Compared with placebo, 'polypills' reduced systolic blood pressure by -9.2 mmHg (95% confidence interval (CI): -13.4, -5.0) diastolic blood pressure by -5.0 mmHg (95%CI: -7.4, -2.6), total cholesterol by -1.22 mmol/L (95%CI: -1.60, -0.84) and LDL-cholesterol by -1.02 mmol/L (95%CI: -1.37, -0.67). However, those taking a 'polypill' (vs. placebo or component) were more likely to discontinue medication (20% vs 14%) (Odds ratio: 1.5 (95% CI: 1.2, 1.9)). There was no significant difference in reported adverse effects amongst those on a 'polypill' (36% vs. 28%) (OR: 1.3 (95%CI: 0.7, 2.5)). There was high statistical heterogeneity in comparisons for blood pressure and lipid-lowering but use of random-effects and quality-effects models produced very similar results.
Conclusions/significance: Compared with placebo, the 'polypills' reduced blood pressure and lipids. Tolerability was lower amongst those on 'polypills' than those on placebo or one component, but differences were moderate. Effectiveness trials are needed to help clarify the status of 'polypills' in primary care and prevention strategies.
Conflict of interest statement
Figures
References
-
- World Health Organization (2008) The global burden of disease: 2004 update. Geneva: World Health Organization: WHO website. Available: http://www.who.int/healthinfo/global_burden_disease/2004_report_update/e... Accessed: August 2012.
-
- National Institute for Health and Clinical Excellence (2011) Secondary prevention in primary and secondary care for patients following a myocardial infarction. UK: NHS website. Available: http://publications.nice.org.uk/mi-secondary-prevention-cg48/introduction Accessed: 8th June 2012.
-
- New Zealand Guidelines Group (2012) New Zealand Primary Care Handbook 2012: Cardiovascular risk assessment and diabetes screening; Cardiovascular risk factor management; Management of type 2 diabetes. NZGG website. Available: http://www.health.govt.nz/publication/new-zealand-primary-care-handbook-... Accessed: November 2012.
