

Can particulate air sampling predict microbial load in operating theatres for arthroplasty?
- PMID: 23285189
- PMCID: PMC3528722
- DOI: 10.1371/journal.pone.0052809
Can particulate air sampling predict microbial load in operating theatres for arthroplasty?
Abstract
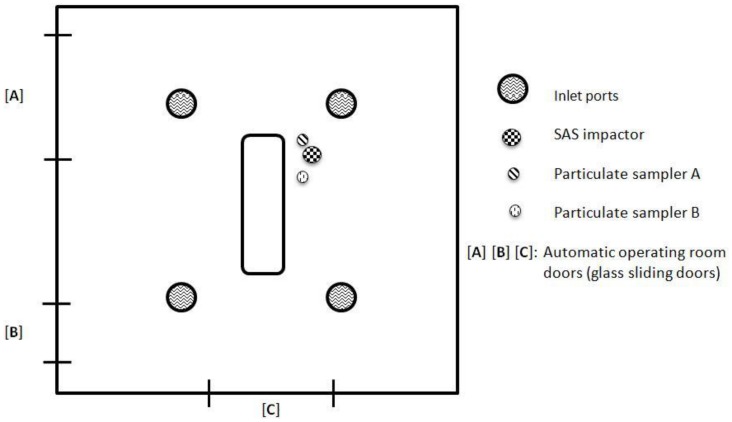
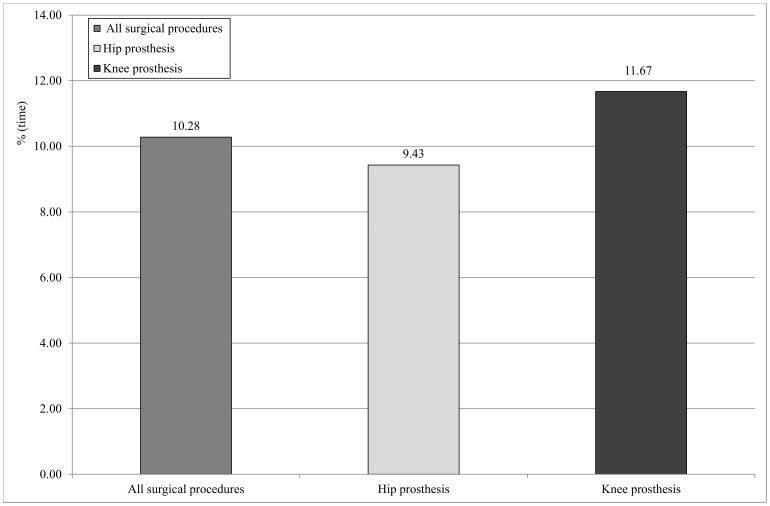
Several studies have proposed that the microbiological quality of the air in operating theatres be indirectly evaluated by means of particle counting, a technique derived from industrial clean-room technology standards, using airborne particle concentration as an index of microbial contamination. However, the relationship between particle counting and microbiological sampling has rarely been evaluated and demonstrated in operating theatres. The aim of the present study was to determine whether particle counting could predict microbiological contamination of the air in an operating theatre during 95 surgical arthroplasty procedures. This investigation was carried out over a period of three months in 2010 in an orthopedic operating theatre devoted exclusively to prosthetic surgery. During each procedure, the bacterial contamination of the air was determined by means of active sampling; at the same time, airborne particulate contamination was assessed throughout the entire procedure. On considering the total number of surgical operations, the mean value of the total bacterial load in the center of the operating theatre proved to be 35 CFU/m(3); the mean particle count was 4,194,569 no./m(3) for particles of diameter ≥0.5 µm and 13,519 no./m(3) for particles of diameter ≥5 µm. No significant differences emerged between the median values of the airborne microbial load recorded during the two types of procedure monitored. Particulates with a diameter of ≥0.5 µm were detected in statistically higher concentrations (p<0.001) during knee-replacement procedures. By contrast, particulates with a diameter of ≥5 µm displayed a statistically higher concentration during hip-replacement procedures (p<0.05). The results did not reveal any statistically significant correlation between microbial loads and particle counts for either of the particle diameters considered (≥0.5 µm and ≥5 µm). Consequently, microbiological monitoring remains the most suitable method of evaluating the quality of air in operating theatres.
Conflict of interest statement
Figures
References
-
- Al-Waked R (2010) Effect of Ventilation Strategies on Infection Control inside Operating Theatres. Eng Appl Comp Fluid 4: 1–16.
-
- Andersson AE, Bergh I, Karlsson J, Eriksson BI, Nilsson K (2012) Traffic flow in the operating room: An explorative and descriptive study on air quality during orthopedic trauma implant surgery. Am J Infect Control 40: 750–755. - PubMed
-
- Dharan S, Pittet D (2002) Environmental controls in operating theatres. J Hosp Infect 51: 79–84. - PubMed
-
- Weaving P, Cox F, Milton S (2008) Infection prevention and control in the operating theatre: reducing the risk of surgical site infections (SSIs). J Perioper Pract 18: 199–204. - PubMed
-
- Gould D (2001) Clean surgical wounds: prevention of infection. Nurs Stand 15: 45–52. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
