

Early clinical and subclinical visual evoked potential and Humphrey's visual field defects in cryptococcal meningitis
- PMID: 23285220
- PMCID: PMC3528708
- DOI: 10.1371/journal.pone.0052895
Early clinical and subclinical visual evoked potential and Humphrey's visual field defects in cryptococcal meningitis
Abstract
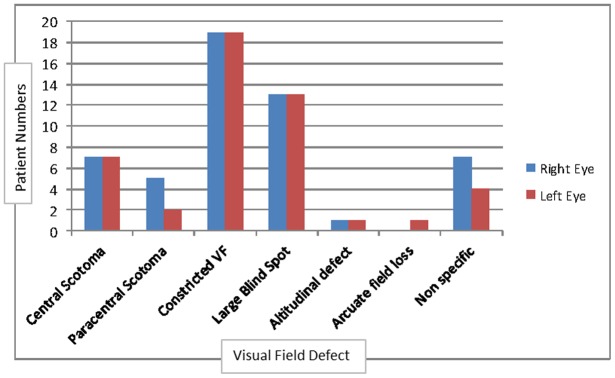
Cryptococcal induced visual loss is a devastating complication in survivors of cryptococcal meningitis (CM). Early detection is paramount in prevention and treatment. Subclinical optic nerve dysfunction in CM has not hitherto been investigated by electrophysiological means. We undertook a prospective study on 90 HIV sero-positive patients with culture confirmed CM. Seventy-four patients underwent visual evoked potential (VEP) testing and 47 patients underwent Humphrey's visual field (HVF) testing. Decreased best corrected visual acuity (BCVA) was detected in 46.5% of patients. VEP was abnormal in 51/74 (68.9%) right eyes and 50/74 (67.6%) left eyes. VEP P100 latency was the main abnormality with mean latency values of 118.9 (±16.5) ms and 119.8 (±15.7) ms for the right and left eyes respectively, mildly prolonged when compared to our laboratory references of 104 (±10) ms (p<0.001). Subclinical VEP abnormality was detected in 56.5% of normal eyes and constituted mostly latency abnormality. VEP amplitude was also significantly reduced in this cohort but minimally so in the visually unimpaired. HVF was abnormal in 36/47 (76.6%) right eyes and 32/45 (71.1%) left eyes. The predominant field defect was peripheral constriction with an enlarged blind spot suggesting the greater impact by raised intracranial pressure over that of optic neuritis. Whether this was due to papilloedema or a compartment syndrome is open to further investigation. Subclinical HVF abnormalities were minimal and therefore a poor screening test for early optic nerve dysfunction. However, early optic nerve dysfunction can be detected by testing of VEP P100 latency, which may precede the onset of visual loss in CM.
Conflict of interest statement
Figures
References
-
- Moosa MY, Coovadia YM (1997) Cryptococcal meningitis in Durban, South Africa: a comparison of clinical features, laboratory findings, and outcome for human immunodeficiency virus (HIV)-positive and HIV-negative patients. Clin Infect Dis 24: 131–134. - PubMed
-
- Seaton RA, Verma N, Naraqi S, Wembri JP, Warrell DA (1997) Visual loss in immunocompetent patients with Cryptococcus neoformans var. gattii meningitis. Trans R Soc Trop Med Hyg 91: 44–49. - PubMed
-
- Cohen DB, Glasgow BJ (1993) Bilateral optic nerve cryptococcosis in sudden blindness in patients with acquired immune deficiency syndrome. Ophthalmology 100: 1689–1694. - PubMed
-
- Lipson BK, Freeman WR, Beniz J, Goldbaum MH, Hesselink JR, et al. (1989) Optic neuropathy associated with cryptococcal arachnoiditis in AIDS patients. Am J Ophthalmol 107: 523–527. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
