

Influence of pentraxin 3 (PTX3) genetic variants on myocardial infarction risk and PTX3 plasma levels
- PMID: 23285251
- PMCID: PMC3532160
- DOI: 10.1371/journal.pone.0053030
Influence of pentraxin 3 (PTX3) genetic variants on myocardial infarction risk and PTX3 plasma levels
Abstract
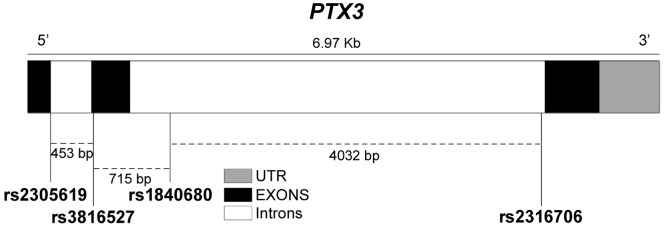
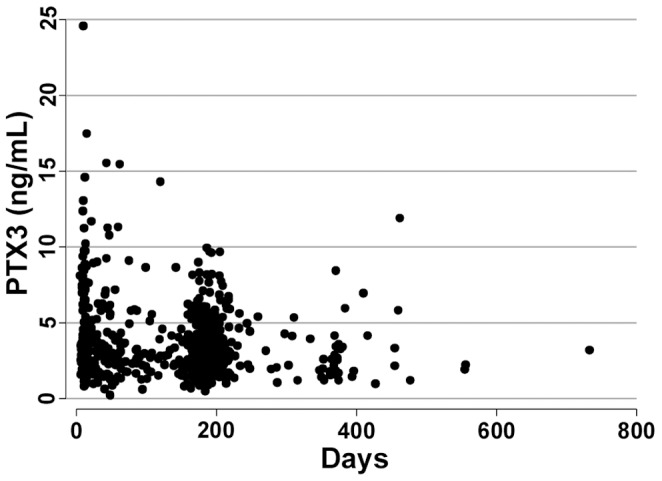
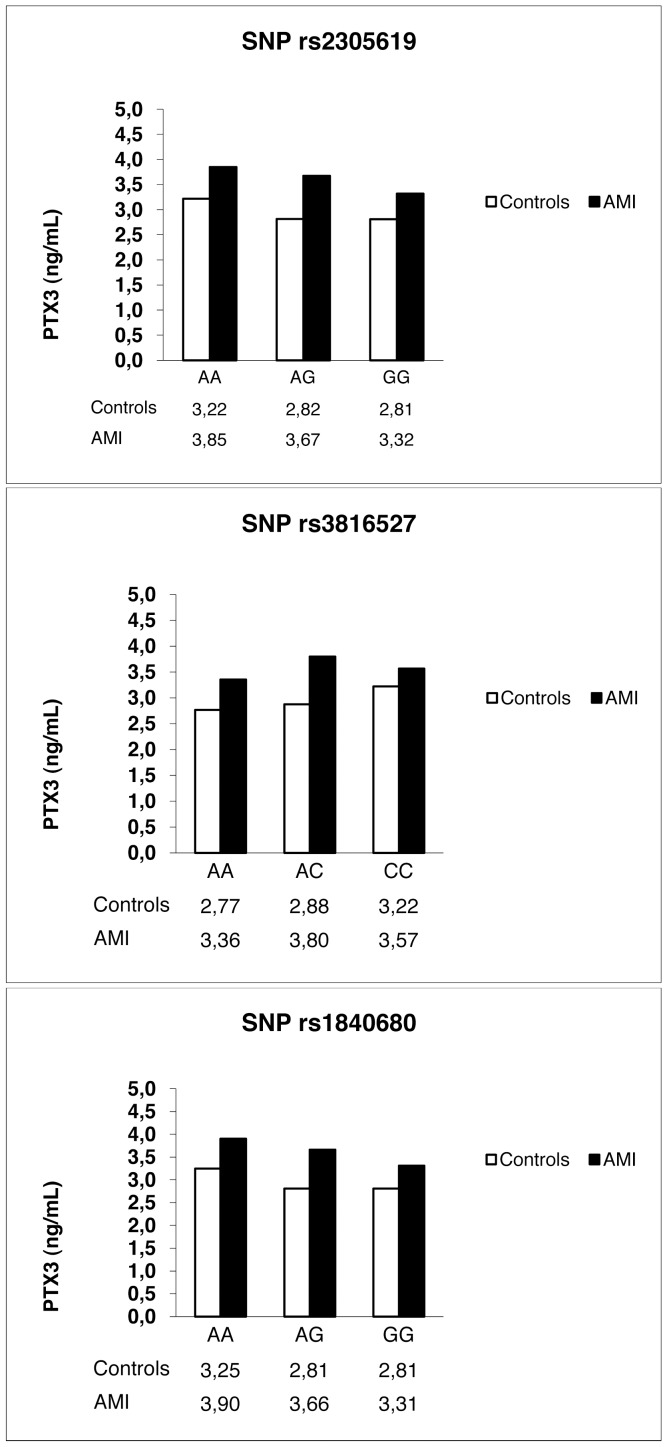
PTX3 is a long pentraxin of the innate immune system produced by different cell types (mononuclear phagocytes, dendritic cells, fibroblasts and endothelial cells) at the inflammatory site. It appears to have a cardiovascular protective function by acting on the immune-inflammatory balance in the cardiovascular system. PTX3 plasma concentration is an independent predictor of mortality in patients with acute myocardial infarction (AMI) but the influence of PTX3 genetic variants on PTX3 plasma concentration has been investigated very little and there is no information on the association between PTX3 variations and AMI. Subjects of European origin (3245, 1751 AMI survivors and 1494 controls) were genotyped for three common PTX3 polymorphisms (SNPs) (rs2305619, rs3816527, rs1840680). Genotype and allele frequencies of the three SNPs and the haplotype frequencies were compared for the two groups. None of the genotypes, alleles or haplotypes were significantly associated with the risk of AMI. However, analysis adjusted for age and sex indicated that the three PTX3 SNPs and the corresponding haplotypes were significantly associated with different PTX3 plasma levels. There was also a significant association between PTX3 plasma concentrations and the risk of all-cause mortality at three years in AMI patients (OR 1.10, 95% CI: 1.01-1.20, p = 0.02). Our study showed that PTX3 plasma levels are influenced by three PTX3 polymorphisms. Genetically determined high PTX3 levels do not influence the risk of AMI, suggesting that the PTX3 concentration itself is unlikely to be even a modest causal factor for AMI. Analysis also confirmed that PTX3 is a prognostic marker after AMI.
Conflict of interest statement
Figures
Similar articles
-
Pentraxin 3 Gene Polymorphisms and Pulmonary Aspergillosis in Chronic Obstructive Pulmonary Disease Patients.Clin Infect Dis. 2018 Jan 6;66(2):261-267. doi: 10.1093/cid/cix749. Clin Infect Dis. 2018. PMID: 29020397
-
rs1840680 single nucleotide polymorphism in Pentraxin 3: a potential protective biomarker of severe community-acquired pneumonia.J Int Med Res. 2021 Apr;49(4):3000605211010621. doi: 10.1177/03000605211010621. J Int Med Res. 2021. PMID: 33906523 Free PMC article.
-
Association of PTX3 Genetic Variants With Development of Diabetic Neuropathy.In Vivo. 2025 Mar-Apr;39(2):702-712. doi: 10.21873/invivo.13874. In Vivo. 2025. PMID: 40010961 Free PMC article.
-
[Pentraxin 3].Rinsho Byori. 2011 Jul;59(7):694-701. Rinsho Byori. 2011. PMID: 21874796 Review. Japanese.
-
[The role of long pentraxin 3, a new inflammatory mediator in inflammatory responses].Nihon Rinsho Meneki Gakkai Kaishi. 2006 Jun;29(3):107-13. doi: 10.2177/jsci.29.107. Nihon Rinsho Meneki Gakkai Kaishi. 2006. PMID: 16819259 Review. Japanese.
Cited by
-
The Long Pentraxin PTX3 as a Link Between Innate Immunity, Tissue Remodeling, and Cancer.Front Immunol. 2019 Apr 4;10:712. doi: 10.3389/fimmu.2019.00712. eCollection 2019. Front Immunol. 2019. PMID: 31019517 Free PMC article. Review.
-
Association of genetic variants of pentraxin 3 rs3816527 with hypertension in Chronic kidney disease patients.Mol Cell Biochem. 2017 Jan;425(1-2):203-212. doi: 10.1007/s11010-016-2874-z. Epub 2016 Nov 12. Mol Cell Biochem. 2017. PMID: 27838804
-
Epigenetic regulation of the extrinsic oncosuppressor PTX3 gene in inflammation and cancer.Oncoimmunology. 2017 May 30;6(7):e1333215. doi: 10.1080/2162402X.2017.1333215. eCollection 2017. Oncoimmunology. 2017. PMID: 28811977 Free PMC article.
-
The Long Pentraxin PTX3 as a Humoral Innate Immunity Functional Player and Biomarker of Infections and Sepsis.Front Immunol. 2019 Apr 12;10:794. doi: 10.3389/fimmu.2019.00794. eCollection 2019. Front Immunol. 2019. PMID: 31031772 Free PMC article. Review.
-
Interleukin 6 (rs1800795) and pentraxin 3 (rs2305619) polymorphisms-association with inflammation and all-cause mortality in end-stage-renal disease patients on dialysis.Sci Rep. 2021 Jul 20;11(1):14768. doi: 10.1038/s41598-021-94075-x. Sci Rep. 2021. PMID: 34285273 Free PMC article.
References
-
- Dahlof B (2010) Cardiovascular disease risk factors: epidemiology and risk assessment. The American Journal of Cardiology 105: 3A–9A. - PubMed
-
- Lloyd-Jones DM (2010) Cardiovascular risk prediction: basic concepts, current status, and future directions. Circulation 121: 1768–1777. - PubMed
-
- Hansson GK, Hermansson A (2011) The immune system in atherosclerosis. Nature immunology 12: 204–212. - PubMed
-
- Hansson GK (2005) Inflammation, atherosclerosis, and coronary artery disease. The New England Journal of Medicine 352: 1685–1695. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
