

Integration of HIV care and treatment in primary health care centers and patient retention in central Mozambique: a retrospective cohort study
- PMID: 23288031
- PMCID: PMC4551421
- DOI: 10.1097/QAI.0b013e3182840d4e
Integration of HIV care and treatment in primary health care centers and patient retention in central Mozambique: a retrospective cohort study
Abstract
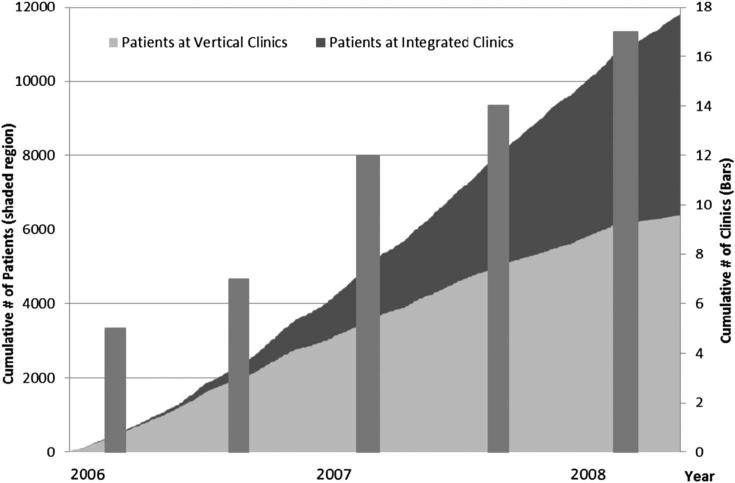
Background: In 2004, the Mozambican Ministry of Health began a national scale-up of antiretroviral therapy (ART) using a vertical model of HIV clinics colocated within large urban hospitals. In 2006, the ministry expanded access by integrating ART into primary health care clinics.
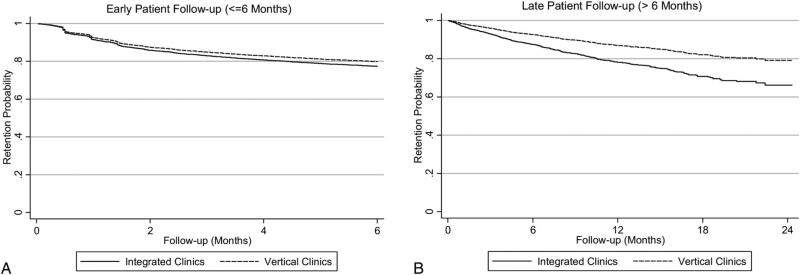
Methods: We conducted a retrospective cohort study including adult ART-naive patients initiating ART between January 2006 and June 2008 in public sector clinics in Manica and Sofala provinces. Cox proportional hazards models with robust variances were used to estimate the association between clinic model (vertical/integrated), clinic location (urban/rural), and clinic experience (first 6 months/post first 6 months) and attrition occurring in early patient follow-up (≤ 6 months) and attrition occurring in late patient follow-up (>6 months), while controlling for age, sex, education, pre-ART CD4 count, World Health Organization stage and pharmacy staff burden.
Results: A total of 11,775 patients from 17 clinics were studied. The overall attrition rate was 37 per 100 person-years. Patients attending integrated clinics had a higher risk of attrition in late follow-up [hazard ratio (HR) = 1.75; 95% confidence interval (CI): 1.04 to 2.94], and patients attending urban clinics (HR = 0.57; 95% CI: 0.35 to 0.91) had a lower risk of attrition in late follow-up. Though not statistically significant, clinics open for longer than 6 months (HR = 0.71; 95% CI: 0.49 to 1.04) had a lower risk of attrition in early follow-up.
Conclusions: Patients attending vertical clinics had a lower risk of attrition. Utilizing primary health clinics to implement ART is necessary to reach higher levels of coverage; however, further implementation strategies should be developed to improve patient retention in these settings.
Figures
References
-
- UNAIDS [January 31, 2012];AIDS at 30: nations at the crossroads. 2011 Available at: http://www.unaids.org/unaids_resources/aidsat30/aids-at-30.pdf.
-
- WHO/UNAIDS Global HIV/AIDS response—epidemic update and health sector progress towards universal access: progress report 2011. 2011:1–223. Available at: http://whqlibdoc.who.int/publications/2011/9789241502986_eng.pdf. February 2, 2012.
-
- Pfeiffer J, Montoya P, Baptista AJ, et al. Integration of HIV/AIDS services into African primary health care: lessons learned for health system strengthening in Mozambique—a case study. [January 31, 2012];J Int AIDS Soc. 2010 13:3. Available at: http://www.pubmedcentral.nih.gov/articlerender.fcgiartid=2828398&tool=pm.... - PMC - PubMed
-
- Stringer JSA, Zulu I, Levy J, et al. Rapid scale-up of antiretroviral therapy at primary care sites in Zambia: feasibility and early outcomes. [August 18, 2011];JAMA. 2006 296:782–793. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16905784. - PubMed
-
- Chan AK, Mateyu G, Jahn A, et al. Outcome assessment of decentralization of antiretroviral therapy provision in a rural district of Malawi using an integrated primary care model. [September 25, 2011];Trop Med Int Health. 2010 15(suppl 1):90–97. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20586966. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
