

Optimizing statistical parametric mapping analysis of 18F-FDG PET in children
- PMID: 23289862
- PMCID: PMC3558387
- DOI: 10.1186/2191-219X-3-2
Optimizing statistical parametric mapping analysis of 18F-FDG PET in children
Abstract
Background: Statistical parametric mapping (SPM) procedure is an objective tool to analyze 18F-fluoro-2-deoxy-d-glucose-positron-emission tomography (FDG-PET) images and a useful complement to visual analysis. However, SPM requires a comparison to control data set that cannot be obtained in healthy children for ethical reasons. Using adults as controls showed some limitations. The purpose of the present study was to generate and validate a group of pseudo-normal children as a control group for FDG-PET studies in pediatrics.
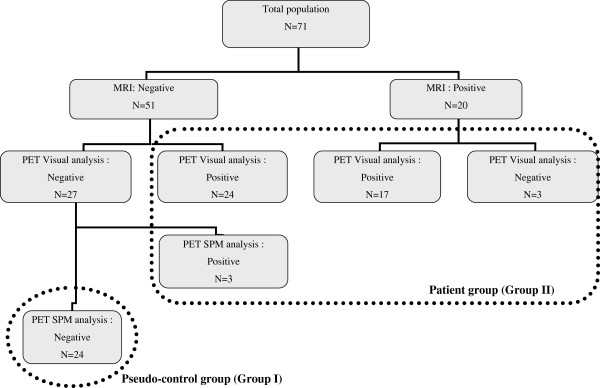
Methods: FDG-PET images of 47 children (mean ± SD age 10.2 ± 3.1 years) with refractory symptomatic (MRI-positive, n = 20) and cryptogenic (MRI-negative, n = 27) focal epilepsy planned for surgery were analyzed using visual and SPM analysis. Performances of SPM analysis were compared using two different control groups: (1) an adult control group consisting of healthy young adults (n = 25, 30.5 ± 5.8 years, adult PET template) and (2) a pediatric pseudo-control group consisting of patients (n = 24, 10.6 ± 3.1 years, children PET template) with refractory focal epilepsy but with negative MRI and with PET considered normal not only on visual analysis but also on SPM.
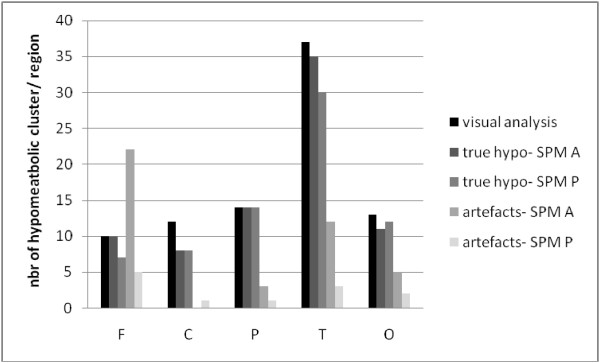
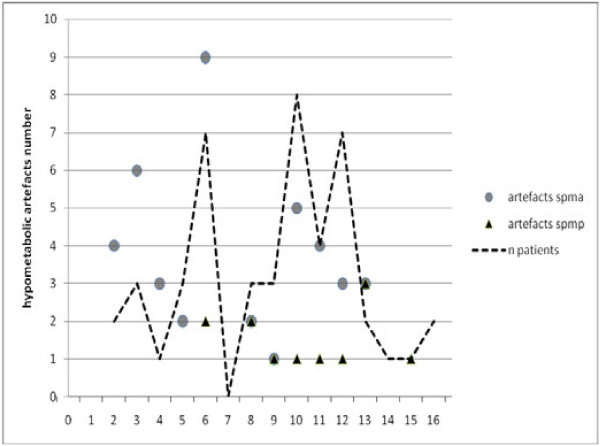
Results: Among the 47 children, visual analysis succeeded detecting at least one hypometabolic area in 87% of the cases (interobserver kappa = 0.81). Regarding SPM analysis, the best compromise between sensitivity and specificity was obtained with a threshold of p less than 0.001 as an extent of more than 40 voxels. There was a significant concordance to detect hypometabolic areas between both SPM analyses [kappa (K) = 0.59; p < 0.005] and between both SPM and visual analyses (K = 0.45; p < 0.005), in symptomatic (K = 0.74; p < 0.005) as in cryptogenic patients (K = 0.26; p < 0.01). The pediatric pseudo-control group dramatically improved specificity (97% vs. 89%; p < 0.0001) by increasing the positive predictive value (86% vs. 65%). Sensitivity remained acceptable although it was not better (79% vs. 87%, p = 0.039). The main impact was to reduce by 41% the number of hypometabolic cortical artifacts detected by SPM, especially in the younger epileptic patients, which is a key point in clinical practice.
Conclusions: This age-matched pseudo-control group is a way to optimize SPM analysis of FDG-PET in children with epilepsy. It might also be considered for other brain pathologies in pediatrics in the future.
Figures
References
-
- Ollenberger GP, Byrne AJ, Berlangieri SU, Rowe CC, Pathmaraj K, Reutens DC, Berkovic SF, Scheffer IE, Scott AM. Assessment of the role of FDG PET in the diagnosis and management of children with refractory epilepsy. Eur J Nucl Med Mol Imaging. 2005;32(11):1311–1316. doi: 10.1007/s00259-005-1844-6. - DOI - PubMed
-
- Chassoux F, Semah F, Bouilleret V, Landre E, Devaux B, Turak B, Nataf F, Roux FX. Metabolic changes and electro-clinical patterns in mesio-temporal lobe epilepsy: a correlative study. Brain. 2004;127(Pt 1):164–174. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
