

Management and outcome of focal low-grade brainstem tumors in pediatric patients: the St. Jude experience
- PMID: 23289916
- PMCID: PMC4349190
- DOI: 10.3171/2012.11.PEDS12317
Management and outcome of focal low-grade brainstem tumors in pediatric patients: the St. Jude experience
Abstract
Object: Whereas diffuse intrinsic pontine gliomas generally have a short symptom duration and more cranial nerve involvement, focal brainstem gliomas are commonly low grade, with fewer cranial neuropathies. Although these phenotypic distinctions are not absolute predictors of outcome, they do demonstrate correlation in most cases. Because there is a limited literature on focal brainstem gliomas in pediatric patients, the objective of this paper was to report the management and outcome of these tumors.
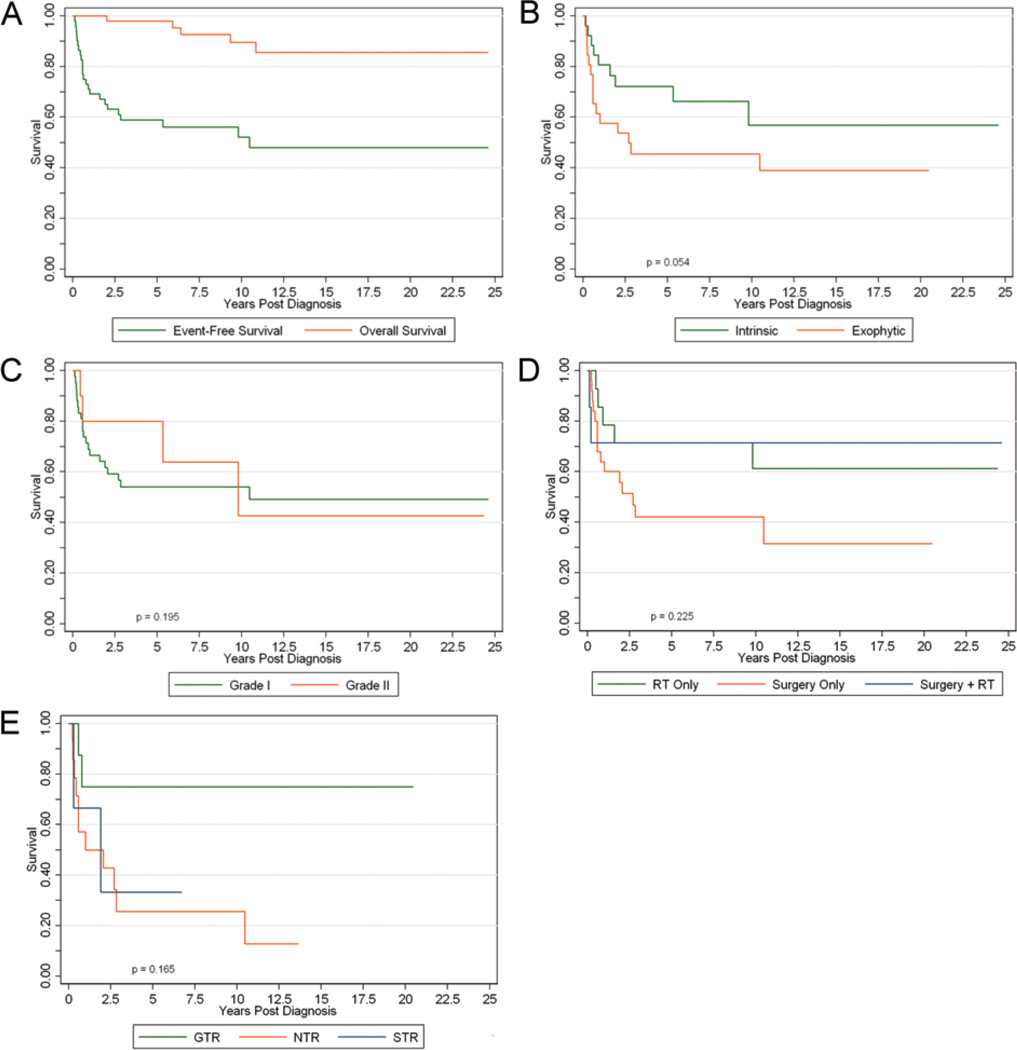
Methods: The authors reviewed the records of all children diagnosed with radiographically confirmed low-grade focal brainstem gliomas from 1986 to 2010. Each patient underwent biopsy or resection for tissue diagnosis. Event-free survival (EFS) and overall survival were evaluated. Univariate analysis was conducted to identify demographic and treatment variables that may affect EFS.
Results: Fifty-two patients (20 girls, 32 boys) with follow-up data were identified. Median follow-up was 10.0 years, and the median age at diagnosis was 6.5 years (range 1-17 years). The tumor locations were midbrain (n = 22, 42%), pons (n = 15, 29%), and medulla (n = 15, 29%). Surgical extirpation was the primary treatment in 25 patients (48%). The 5- and 10-year EFS and overall survival were 59%/98% and 52%/90%, respectively. An event or treatment failure occurred in 24 patients (46%), including 5 deaths. Median time to treatment failure was 3.4 years. Disease progression in the other 19 patients transpired within 25.1 months of diagnosis. Thirteen of these patients received radiation, including 11 within 2 months of primary treatment failure. Although children with intrinsic tumors had slightly better EFS at 5 years compared with those with exophytic tumors (p = 0.054), this difference was not significant at 10 years (p = 0.147). No other variables were predictive of EFS.
Conclusions: Surgery suffices in many children with low-grade focal brainstem gliomas. Radiation treatment is often reserved for disease progression but offers comparable disease control following biopsy. In the authors' experience, combining an assessment of clinical course, imaging, and tumor biopsy yields a reasonable model for managing children with focal brainstem tumors.
Figures
References
-
- Barkovich AJ, Krischer J, Kun LE, Packer R, Zimmerman RA, Freeman CR, et al. Brain stem gliomas: a classification system based on magnetic resonance imaging. Pediatr Neurosurg. 1990–1991;16:73–83. - PubMed
-
- Boydston WR, Sanford RA, Muhlbauer MS, Kun LE, Kirk E, Dohan FC, Jr, et al. Gliomas of the tectum and periaqueductal region of the mesencephalon. Pediatr Neurosurg. 1991–1992;17:234–238. - PubMed
-
- Bricolo A, Turazzi S, Cristofori L, Talacchi A. Direct surgery for brainstem tumours. Acta Neurochir Suppl (Wien) 1991;53:148–158. - PubMed
-
- Choux M, Lena G, Do L. Brainstem tumors. In: Choux M, Di Rocco C, Hockley A, et al., editors. Pediatric Neurosurgery. New York: Churchill Livingstone; 2000. pp. 471–491.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
