

Association of polypectomy techniques, endoscopist volume, and facility type with colonoscopy complications
- PMID: 23290773
- PMCID: PMC4857725
- DOI: 10.1016/j.gie.2012.11.012
Association of polypectomy techniques, endoscopist volume, and facility type with colonoscopy complications
Abstract
Background and objective: Serious GI adverse events in the outpatient setting were examined by polypectomy technique, endoscopist volume, and facility type (ambulatory surgery center and hospital outpatient department).
Design: Retrospective follow-up study.
Setting: Ambulatory surgery and hospital discharge datasets from Florida (1997-2004) were used.
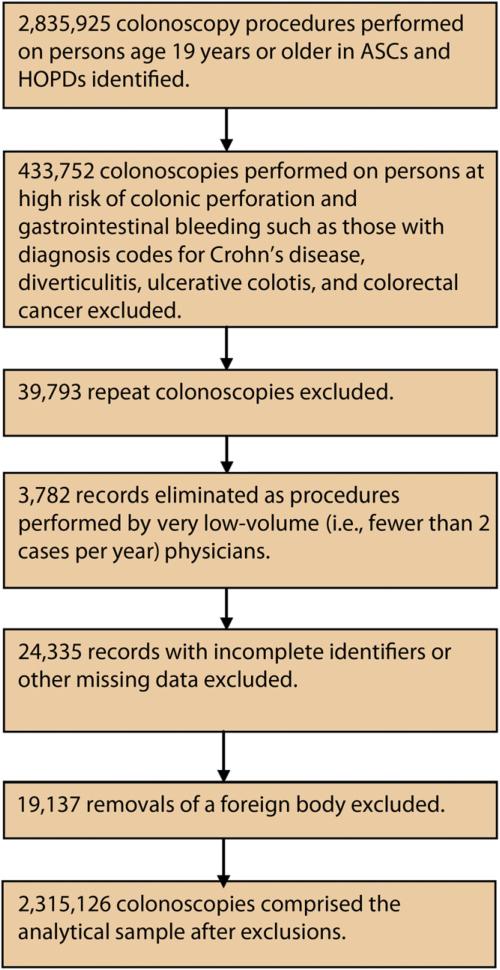
Patients: A total of 2,315,126 outpatient colonoscopies performed in patients of all ages and payers were examined.
Main outcome: Thirty-day hospitalizations because of colonic perforations and GI bleeding, measured as cumulative and specific outcomes, were investigated.
Results: Compared with simple colonoscopy, the adjusted risks of cumulative adverse events were greater with the use of cold forceps (1.21 [95% CI, 1.01-1.44]), ablation (3.75 [95% CI, 2.97-4.72]), hot forceps (5.63 [95% CI, 4.97-6.39]), snares (7.75 [95% CI, 6.95-8.64]), or complex colonoscopy (8.83 [95% CI, 7.70-10.12]). Low-volume endoscopists had higher risks of adverse events (1.18 [95% CI, 1.07-1.30]). A higher risk of adverse events was associated with procedures performed in ambulatory surgery centers (1.27 [95% CI, 1.16-1.40]). Important findings were also reported for the analyses stratified by specific outcomes and procedures.
Limitation: The study was constrained by limitations inherent in administrative data pertaining to a single state.
Conclusions: As the complexity of polypectomy increases, a higher risk of adverse events is reported. Using lower risk procedures when clinically appropriate or referring patients to high-volume endoscopists can reduce the rates of perforations and GI bleeding. Given the large number of colonoscopies performed in the United States, it is critical that the rates of adverse events be considered when choosing procedures.
Copyright © 2013 American Society for Gastrointestinal Endoscopy. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Centers for Disease Control and Prevention Morbidity and Mortality Weekly Report, July 8, 2011. [November 21, 2011];Vital signs: colorectal cancer screening, incidence, and mortality - United States, 2002-2010. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6026a4.htm. - PubMed
-
- Seeff LC, Richards TB, Shapiro JA, et al. How many endoscopies are performed for colorectal cancer screening? Results from CDC's survey of endoscopic capacity. Gastroenterology. 2004;127:1670–7. - PubMed
-
- Levin TR, Zhao W, Conell C, et al. Adverse events of colonoscopy in an integrated health care delivery system. Ann Intern Med. 2006;145:880–6. - PubMed
-
- Singh N, Harrison M, Rex DK. A survey of colonoscopic polypectomy practices among clinical gastroenterologists. Gastrointest Endosc. 2004;60:414–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
