

Combining radiotherapy and cancer immunotherapy: a paradigm shift
- PMID: 23291374
- PMCID: PMC3576324
- DOI: 10.1093/jnci/djs629
Combining radiotherapy and cancer immunotherapy: a paradigm shift
Abstract
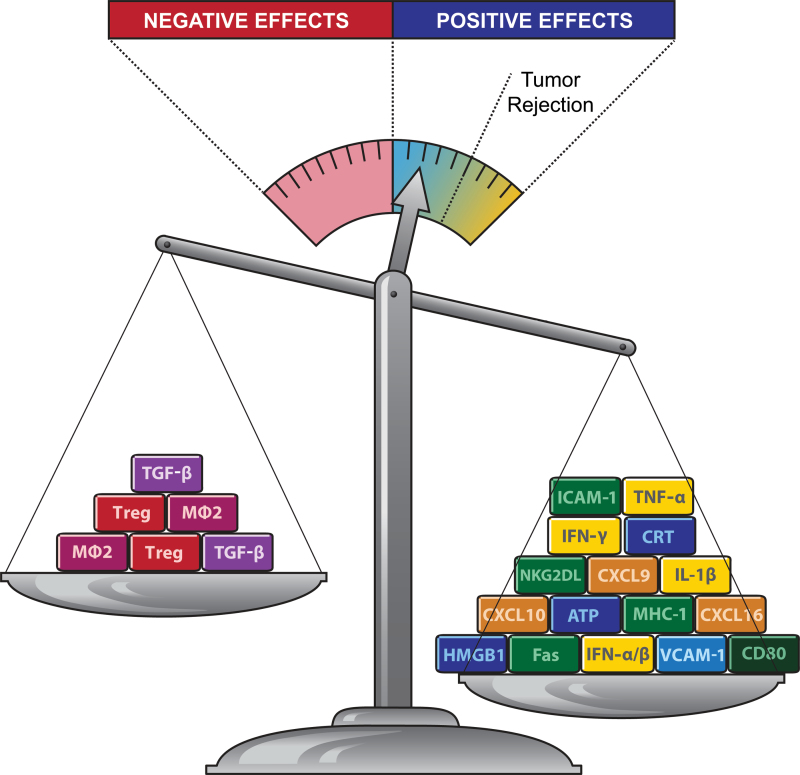
The therapeutic application of ionizing radiation has been largely based on its cytocidal power combined with the ability to selectively target tumors. Radiotherapy effects on survival of cancer patients are generally interpreted as the consequence of improved local control of the tumor, directly decreasing systemic spread. Experimental data from multiple cancer models have provided sufficient evidence to propose a paradigm shift, whereby some of the effects of ionizing radiation are recognized as contributing to systemic antitumor immunity. Recent examples of objective responses achieved by adding radiotherapy to immunotherapy in metastatic cancer patients support this view. Therefore, the traditional palliative role of radiotherapy in metastatic disease is evolving into that of a powerful adjuvant for immunotherapy. This combination strategy adds to the current anticancer arsenal and offers opportunities to harness the immune system to extend survival, even among metastatic and heavily pretreated cancer patients. We briefly summarize key evidence supporting the role of radiotherapy as an immune adjuvant. A critical appraisal of the current status of knowledge must include potential immunosuppressive effects of radiation that can hamper its capacity to convert the irradiated tumor into an in situ, individualized vaccine. Moreover, we discuss some of the current challenges to translate this knowledge to the clinic as more trials testing radiation with different immunotherapies are proposed.
Figures
References
-
- Gough MJ, Crittenden MR. Combination approaches to immunotherapy: the radiotherapy example. Immunotherapy. 2009; 1(6):1025–1037 - PubMed
-
- Hill-Kayser CE, Plastaras JP, Tochner Z, et al. TBI during BM and SCT: review of the past, discussion of the present and consideration of future directions. Bone Marrow Transplant. 2011; 46(4):475–484 - PubMed
-
- Dunn GP, Old LJ, Schreiber RD. The three Es of cancer immunoediting. Annu Rev Immunol. 2004; 22 329–360 - PubMed
-
- Smyth MJ, Dunn GP, Schreiber RD. Cancer immunosurveillance and immunoediting: the roles of immunity in suppressing tumor development and shaping tumor immunogenicity. Adv Immunol. 2006; 90 1–50 - PubMed
-
- Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science. 2011; 331(6024):1565–1570 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
