

Impact of chemotherapy sequencing on local-regional failure risk in breast cancer patients undergoing breast-conserving therapy
- PMID: 23291658
- PMCID: PMC6058313
- DOI: 10.1097/SLA.0b013e3182805c4a
Impact of chemotherapy sequencing on local-regional failure risk in breast cancer patients undergoing breast-conserving therapy
Abstract
Objective: This study was performed to evaluate long-term local-regional control rates after breast-conserving therapy (BCT) for patients undergoing surgery before or after neoadjuvant chemotherapy.
Methods: There were 2983 patients who underwent segmental mastectomy with whole-breast irradiation from 1987 to 2005. Clinicopathological and outcome data were reviewed, and comparisons were made between those undergoing surgery before and those undergoing surgery after neoadjuvant chemotherapy.
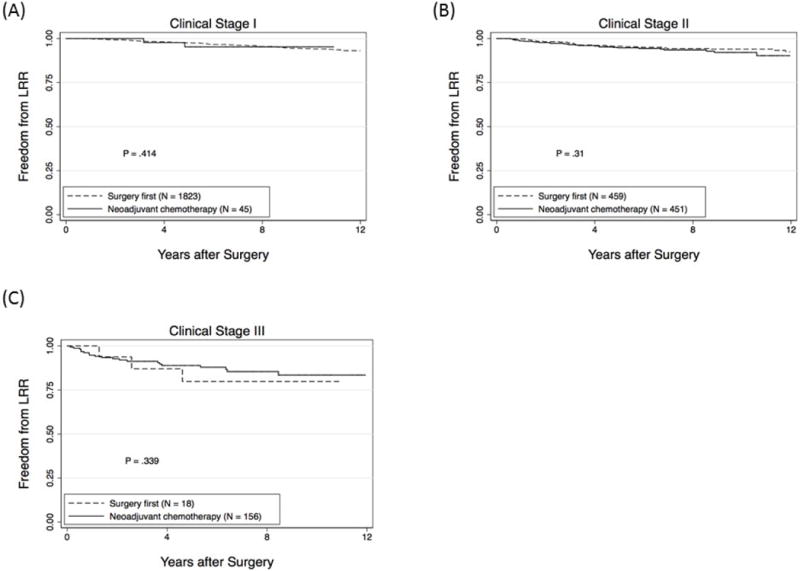
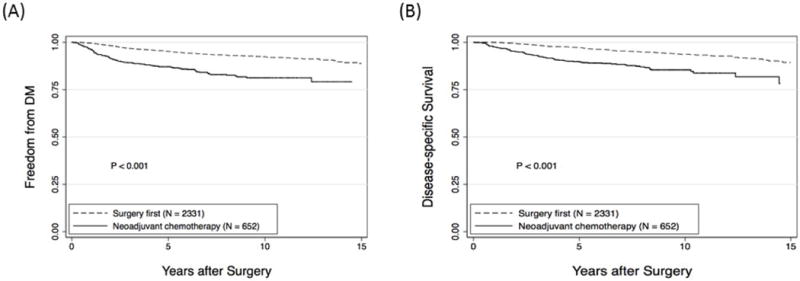
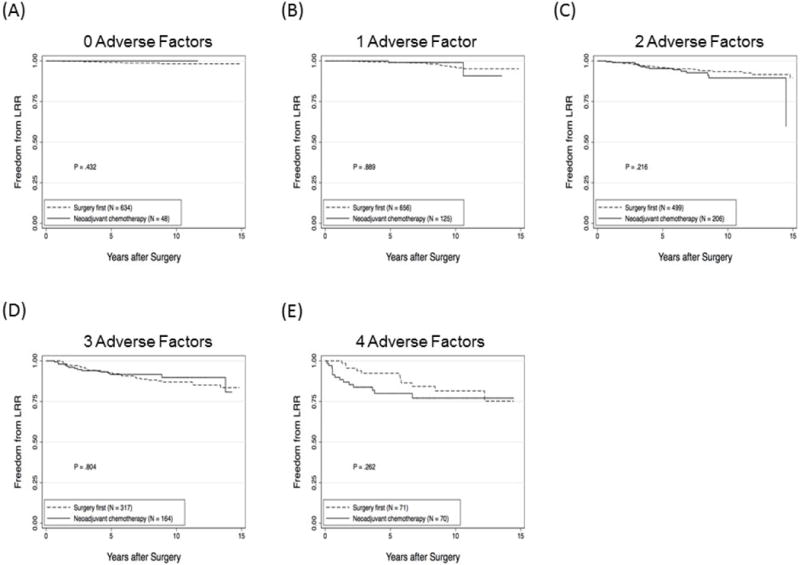
Results: There were 2331 patients (78%) who underwent surgery first and 652 (22%) received neoadjuvant chemotherapy. Patients receiving neoadjuvant chemotherapy had more advanced disease at baseline and more adverse clinicopathological features. The 5- and 10-year local-regional recurrence (LRR)-free survival rates were 97% [95% confidence interval (CI), 96-98) and 94% (95% CI, 93-95) for surgery first and 93% (95% CI, 91-95) and 90% (95% CI, 87-93) after neoadjuvant chemotherapy (P < 0.001). However, there were no differences in LRR-free survival rates when comparing the presenting clinical stage (P = NS). Of 607 patients presenting with clinical stage II/III disease, chemotherapy downstaged 313 patients (52%) to pathological stage 0/I disease; 294 (48%) had residual stage II/III disease. In multivariate analysis, an age less than 50 years, clinical stage III, grade 3, estrogen receptor (ER)-negative disease, estrogen receptor-positive disease without receipt of endocrine therapy, lymphovascular invasion, multifocal disease on pathology, and close/positive margins were associated with LRR. Use of neoadjuvant chemotherapy was not significant when added to the model. Adjusting for adverse factors, there were no differences in LRR between patients who underwent surgery before and those who underwent neoadjuvant chemotherapy after surgery.
Conclusions: LRR after BCT is driven by tumor biology and disease stage. Appropriately selected patients can achieve high rates of local-regional control with BCT with either upfront surgery or surgery after neoadjuvant chemotherapy.
Figures
References
-
- Arriagada R, Le MG, Rochard F, Contesso G. Conservative treatment versus mastectomy in early breast cancer: patterns of failure with 15 years of follow-up data. Institut Gustave-Roussy Breast Cancer Group. J Clin Oncol. 1996;14(5):1558–64. - PubMed
-
- Blichert-Toft M, Rose C, Andersen JA, et al. Danish randomized trial comparing breast conservation therapy with mastectomy: six years of life-table analysis. Danish Breast Cancer Cooperative Group. J Natl Cancer Inst Monogr. 1992;11:19–25. - PubMed
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347(16):1233–41. - PubMed
-
- Poggi MM, Danforth DN, Sciuto LC, et al. Eighteen-year results in the treatment of early breast carcinoma with mastectomy versus breast conservation therapy: the National Cancer Institute Randomized Trial. Cancer. 2003;98(4):697–702. - PubMed
-
- van Dongen JA, Voogd AC, Fentiman IS, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst. 2000;92(14):1143–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
