

Surgical management of primary spinal hemangiopericytomas: an institutional case series and review of the literature
- PMID: 23291785
- PMCID: PMC3641276
- DOI: 10.1007/s00586-012-2626-z
Surgical management of primary spinal hemangiopericytomas: an institutional case series and review of the literature
Erratum in
- Eur Spine J. 2013 May;22 Suppl 3:S460. Banykh, Sergei [corrected to Bannykh, Serguei];Patrick Johnson, J [corrected to Johnson, J P]
Abstract
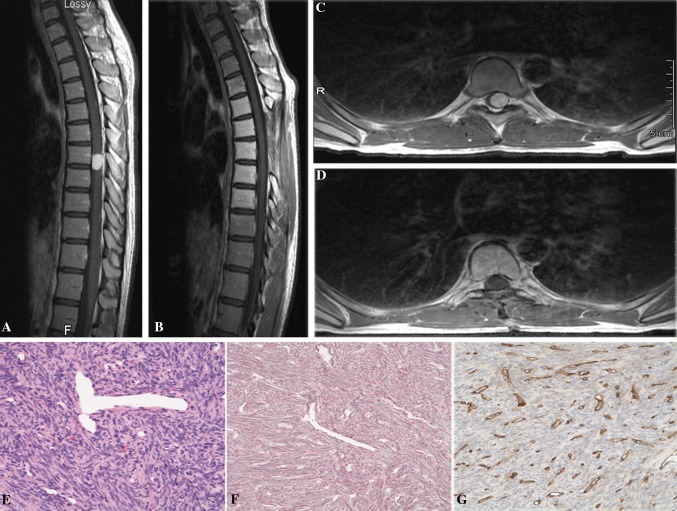
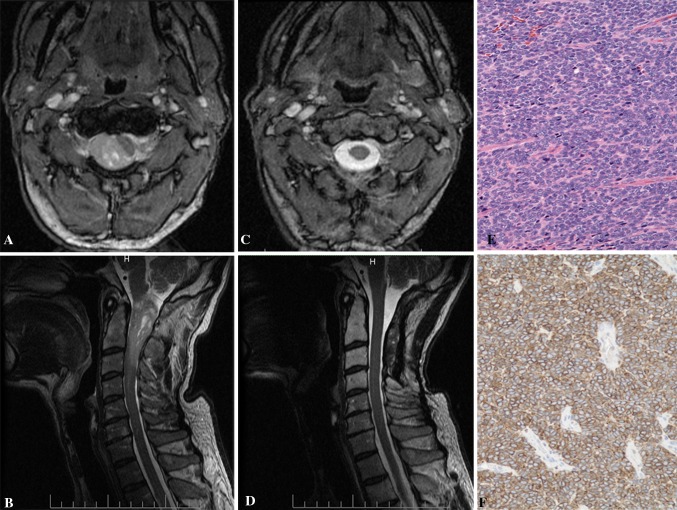
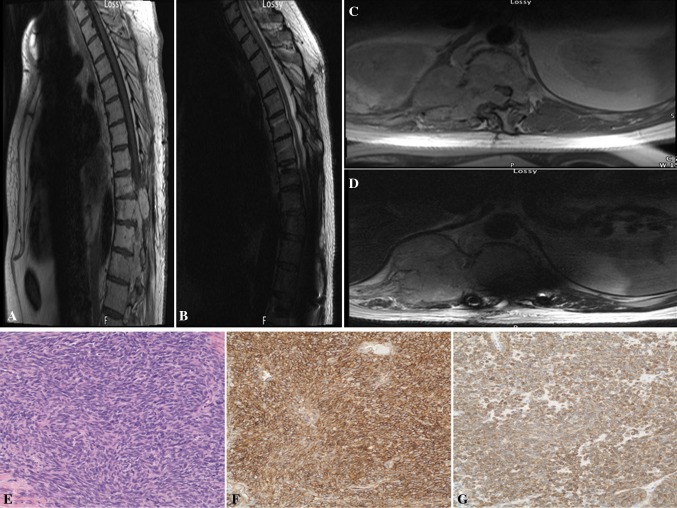
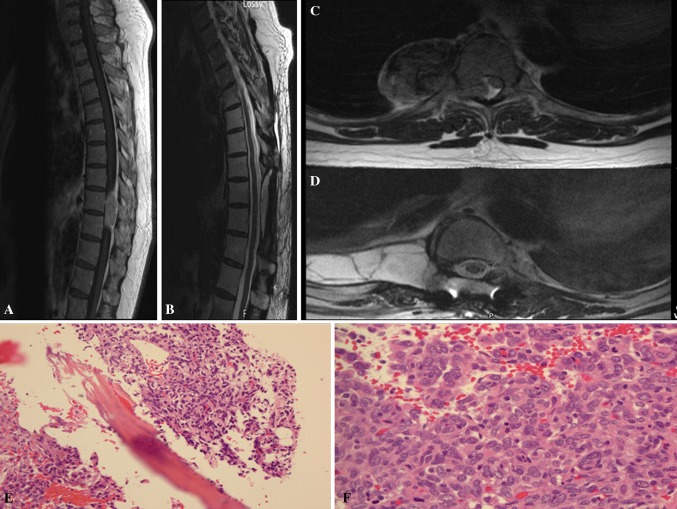
Purpose: Hemangiopericytoma (HPC) is a rare tumor of the central nervous system. Primary spinal occurrence of this tumor is extremely uncommon and cases involving the intramedullary spinal cord are even more rare. The purpose of this study was to explore the clinical features, surgical strategies, outcome and pathology in a consecutive series of patients treated at a single institution.
Methods: The authors performed a retrospective review of the clinicopathological characteristics of four patients with a pathological diagnosis of spinal HPC.
Results: Four cases with intradural as well as intra/extra-medullary components were identified. Gross total resection with no recurrence at the operative site was achieved in the majority of patients with a spinal HPC. One patient had significant recurrence and eventually, succumbed to the disease.
Conclusion: Increased awareness of these tumors' capability to occur intradurally and intramedullarly can help surgeons accurately diagnose and choose an effective plan of care. Gross total resection of hemangiopericytomas is the mainstay of treatment and should be pursued if feasible. Histopathology is essential to the diagnosis.
Figures
References
-
- Giannini C, Rushing EJ, Hainfellner JA. Haemangiopericytoma. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, editors. WHO classification of tumours of the central nervous system. 4. Lyon: International Agency for Research on Cancer (IARC); 2007. pp. 178–180.
-
- Betchen S, Schwartz A, Black C, Post K. Intradural hemangiopericytoma of the lumbar spine: case report. Neurosurgery. 2002;50:654–657. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
